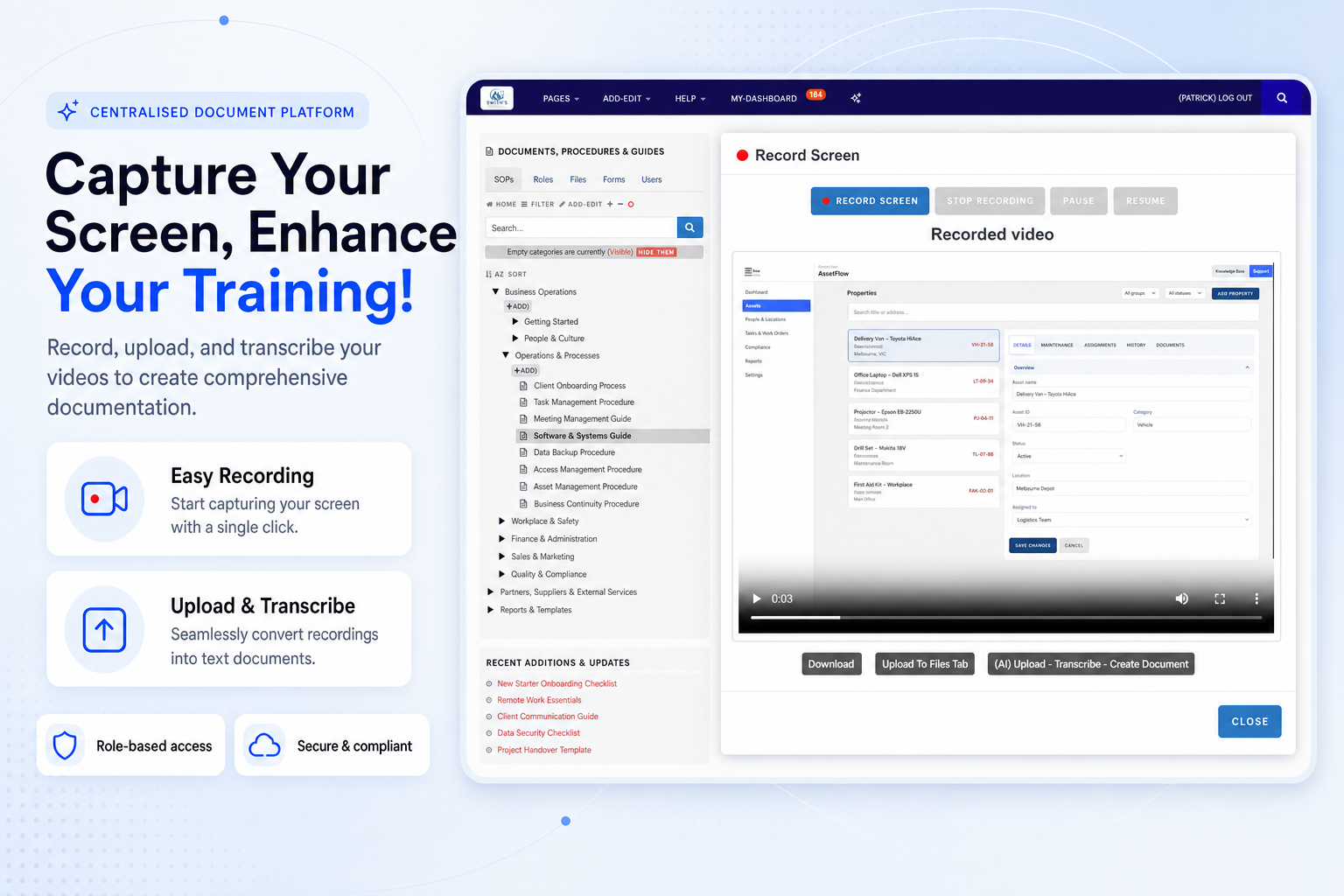
Capture Your Screen, Enhance Your Training
Record important workflows and convert practical know-how into reusable guides, onboarding resources and documented procedures.
Easy recording
Upload and transcribe
End documentation chaos with TKO Guides. Streamline operations, ensure compliance, and boost efficiency across all industries. Book a demo today.
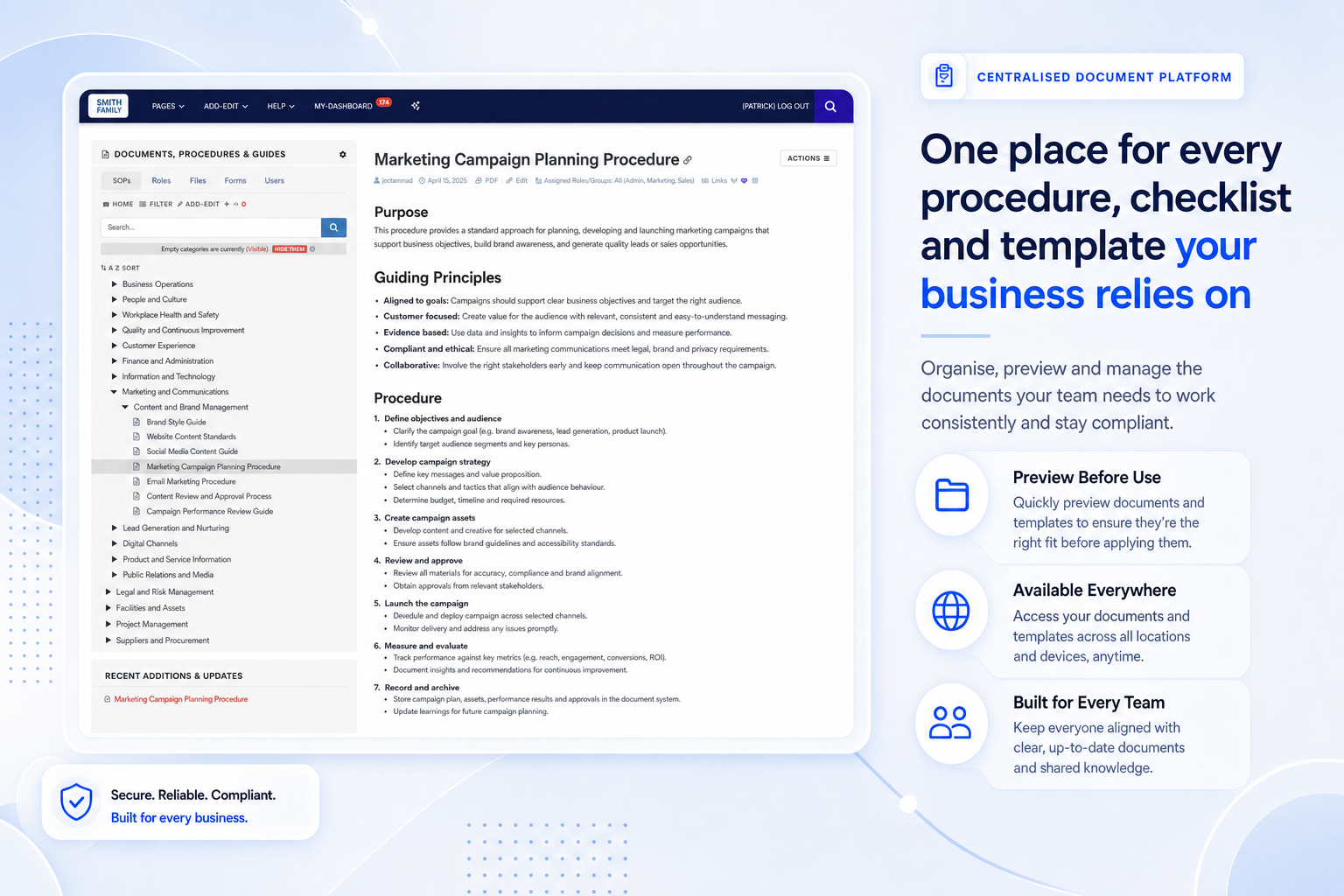
Use TKO’s platform to manage documents seamlessly, ensuring compliance and unhindered productivity across every department and device.
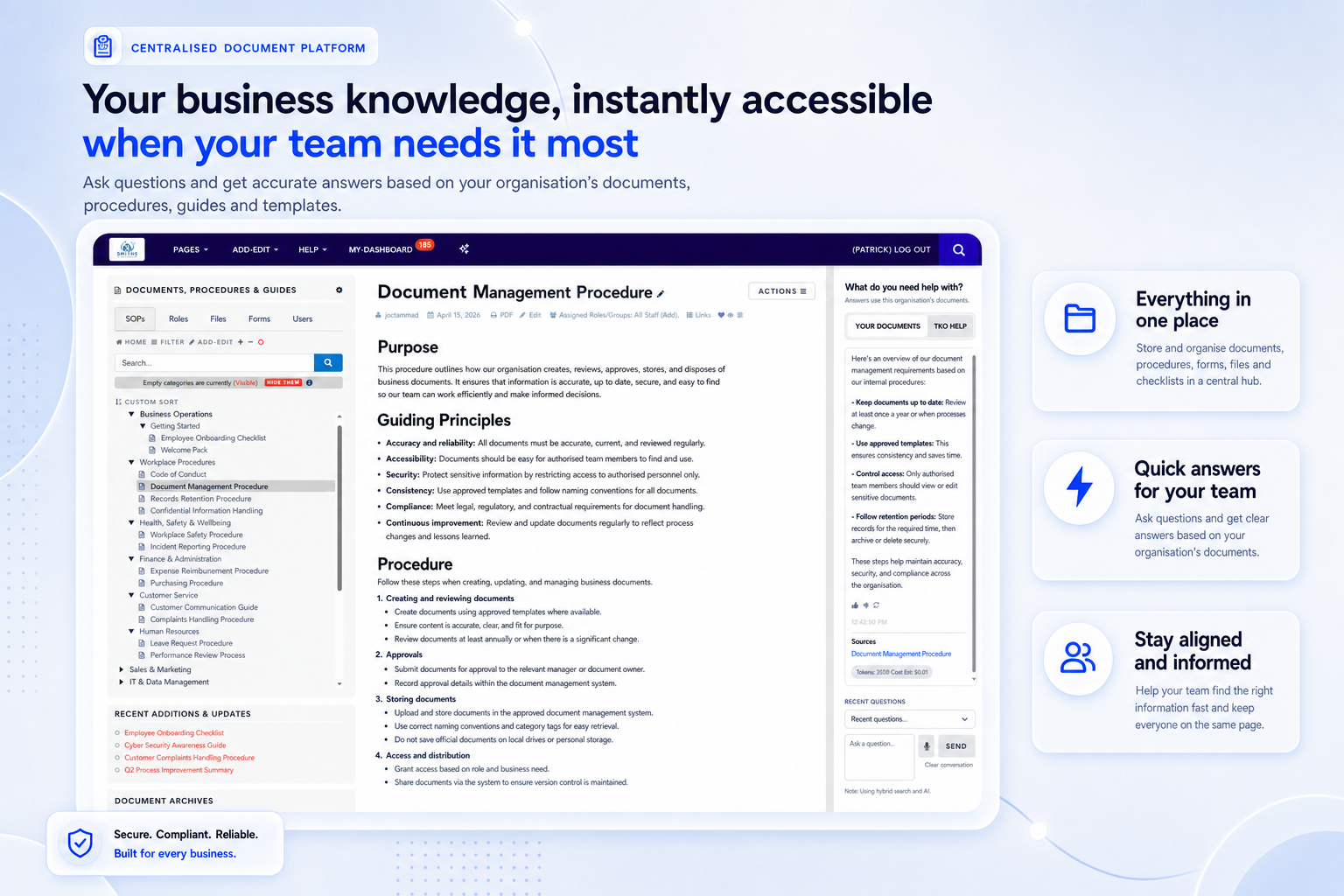
TKO Guides helps organisations replace scattered folders, outdated copies and manual follow-ups with a controlled workspace for SOPs, procedures, forms, training materials and audit evidence.
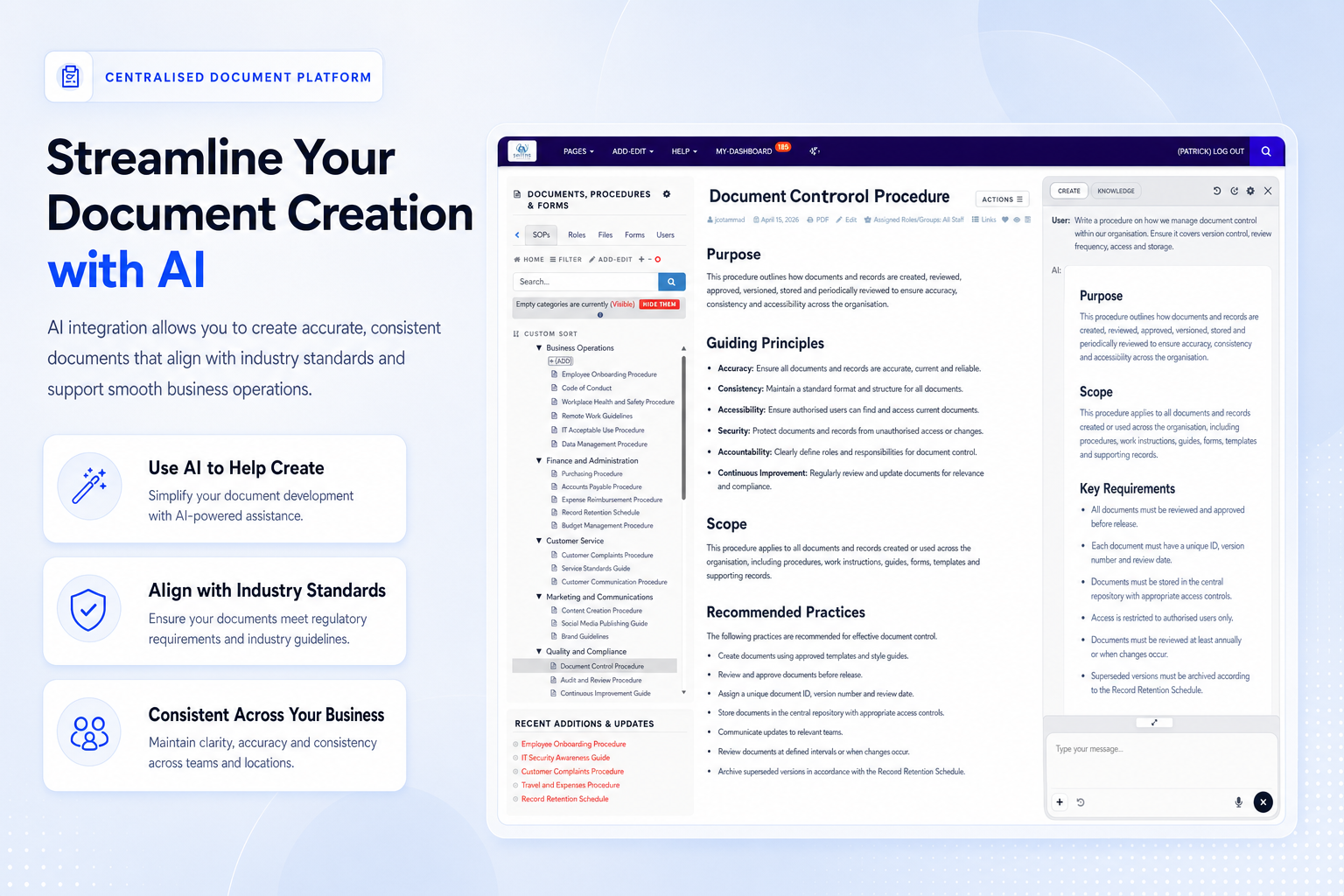
Use intelligent assistance to turn knowledge into structured content, training assets and compliance-ready improvements without slowing daily work.
Record important workflows and convert practical know-how into reusable guides, onboarding resources and documented procedures.
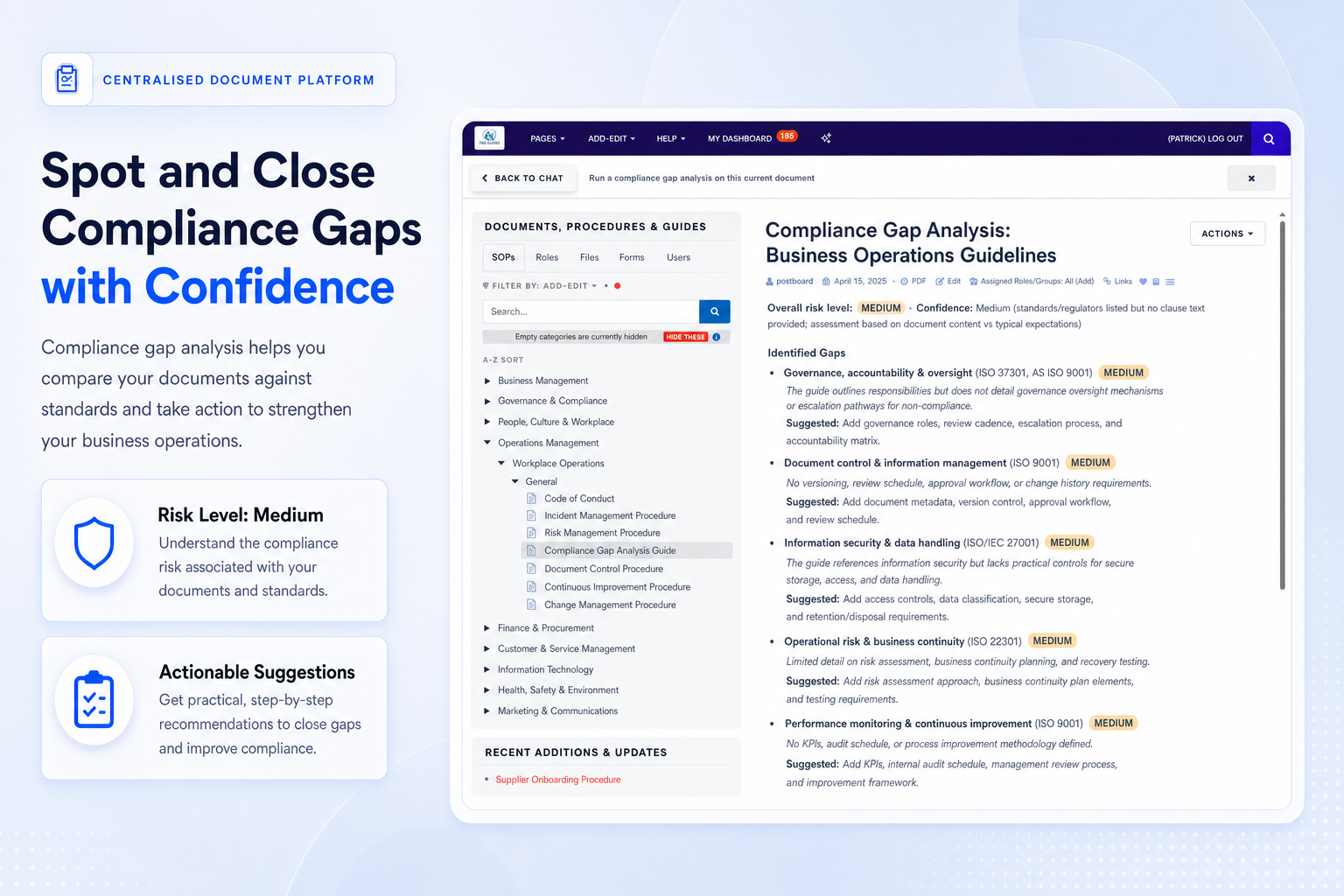
Compare documents against standards, highlight missing evidence and prioritise practical actions before audits or internal reviews.
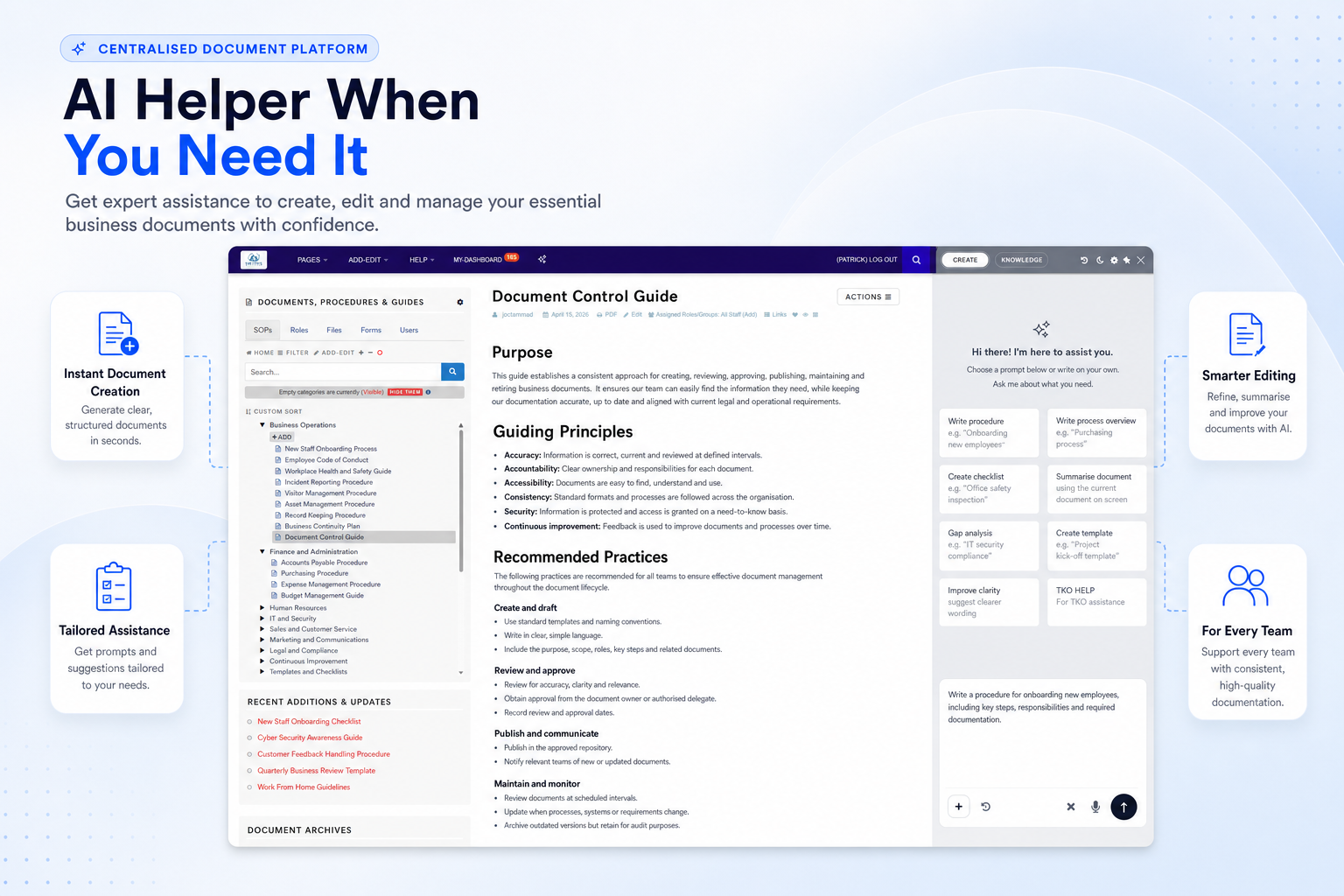
Generate drafts, refine wording and guide document creation with prompts aligned to your operational needs.
See how TKO Guides can help your organisation centralise documents, strengthen audit trails and keep staff aligned with the latest requirements.
Book a DemoFrom creation and review to role assignment, acknowledgements and evidence retrieval, TKO Guides supports the full document lifecycle.
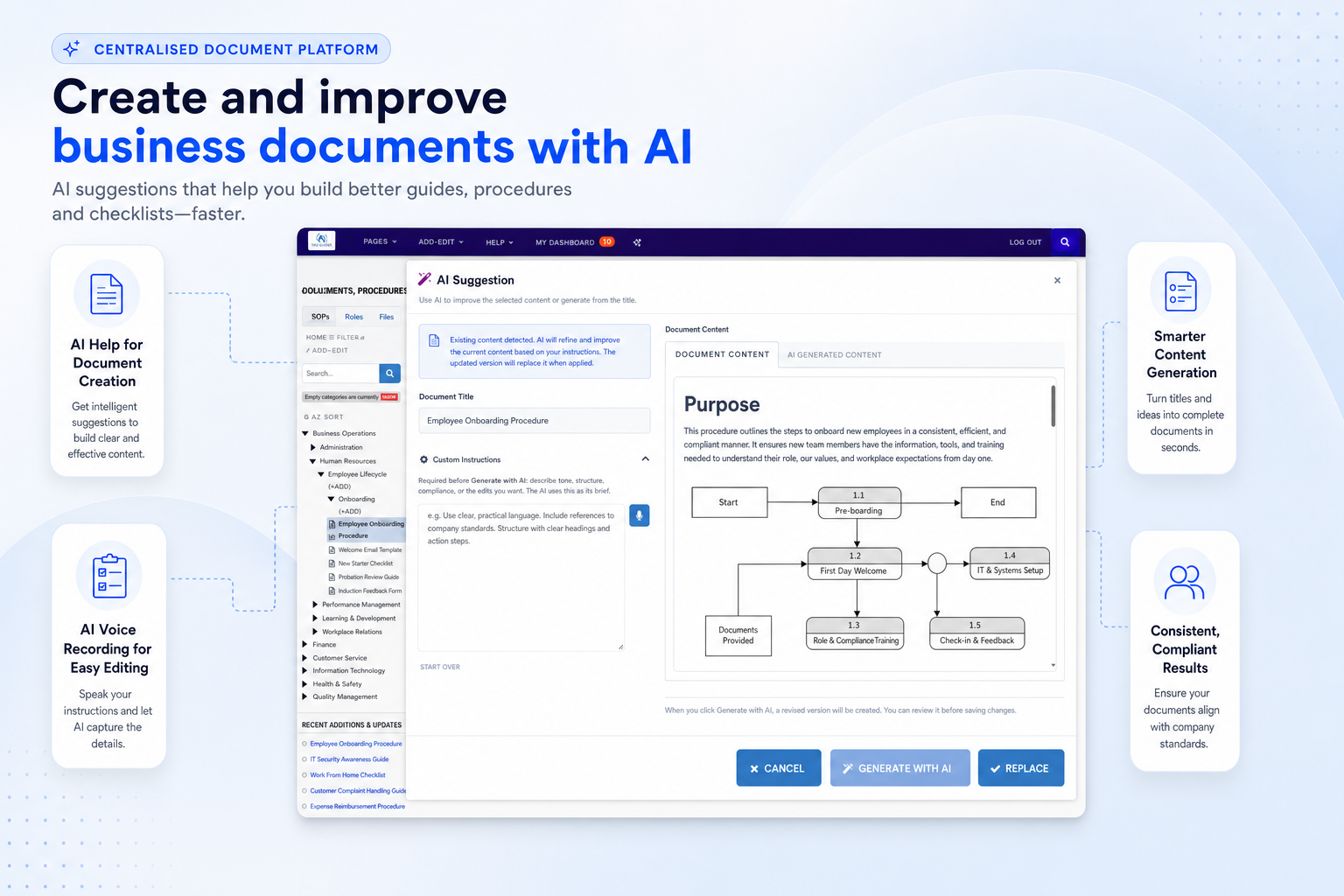
Refine existing content, capture instructions by voice and improve documents with intelligent suggestions.
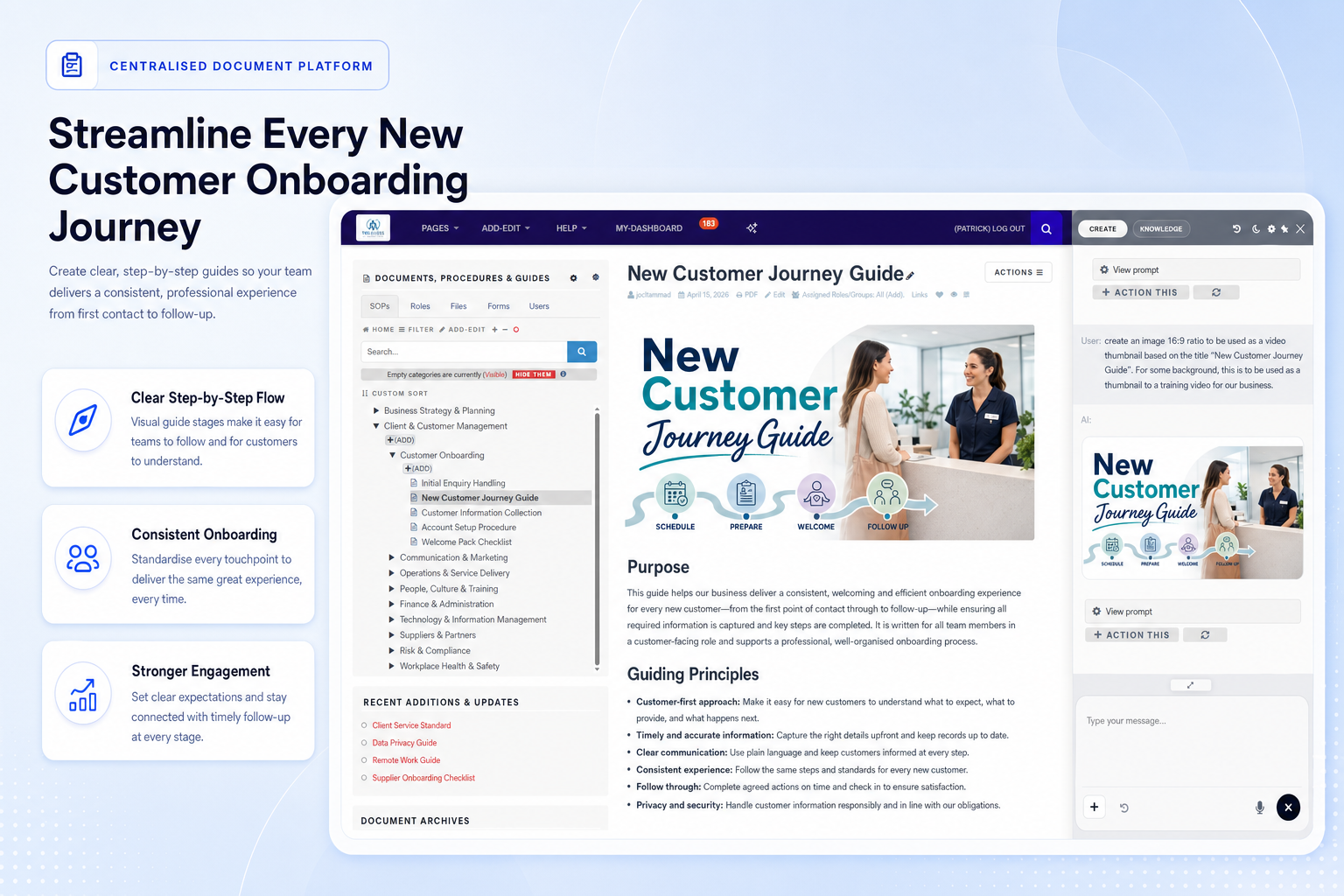
Create clearer guides with visual support so participants, clients and staff understand each step.
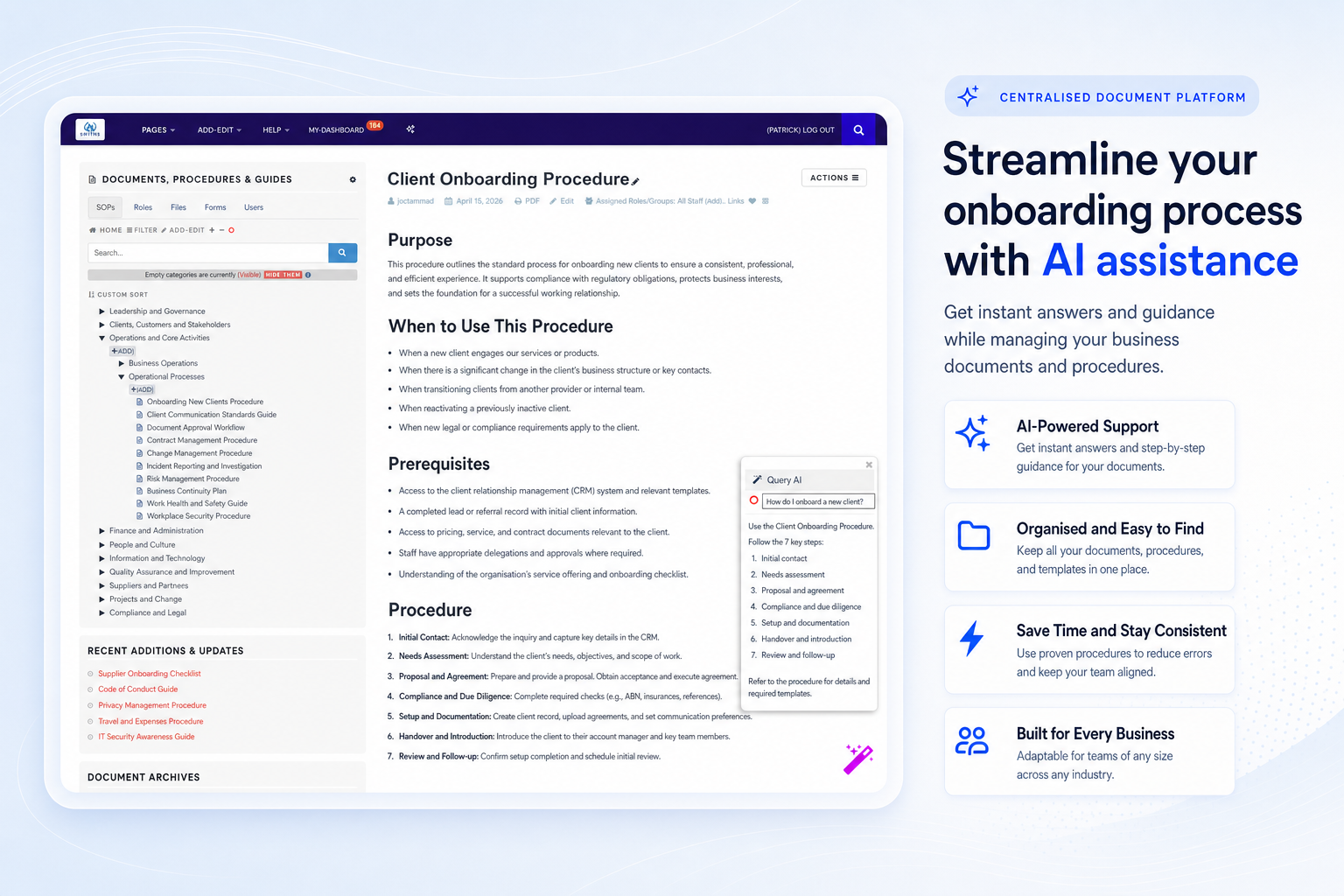
Ask questions in context and retrieve guidance quickly without leaving the document workspace.
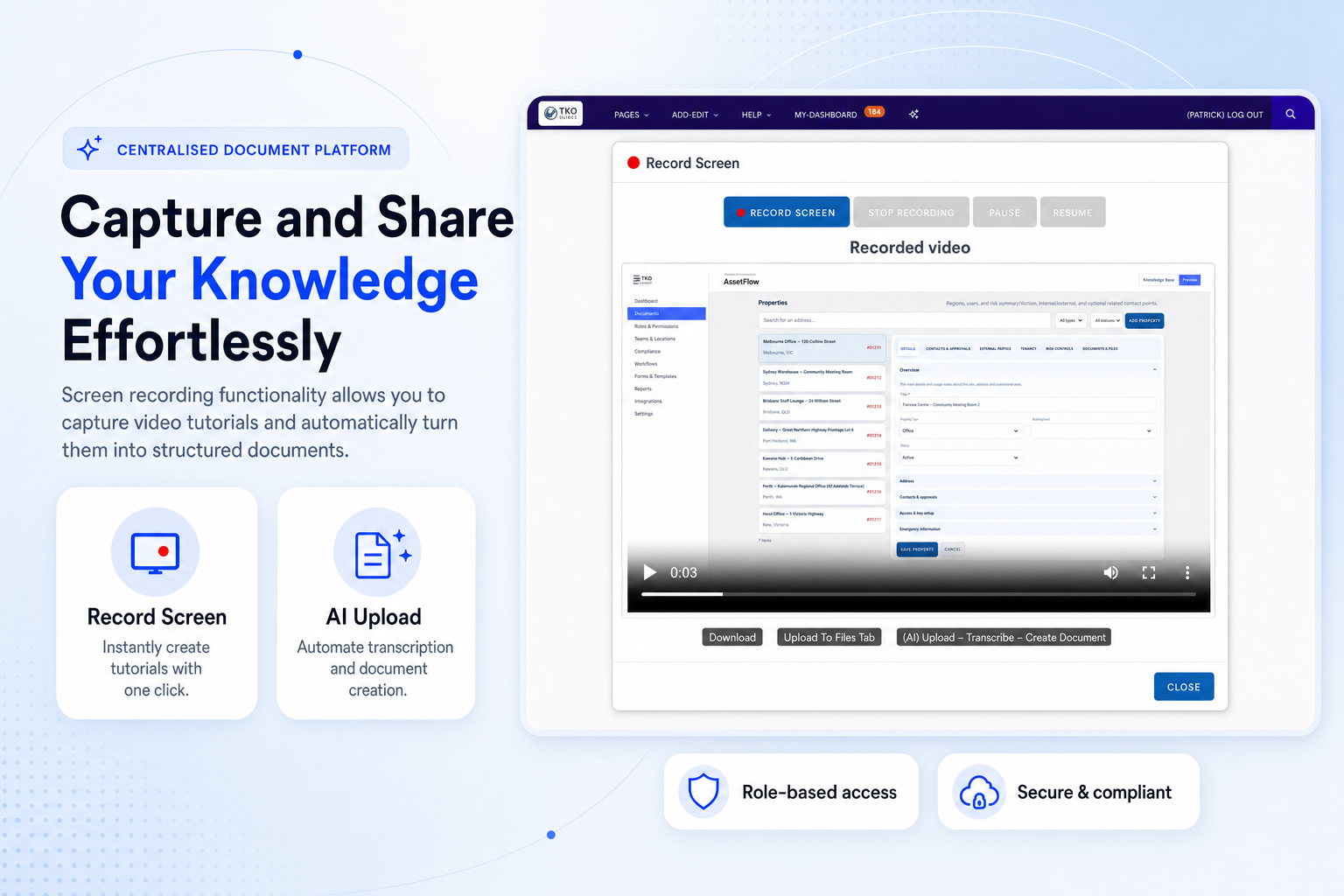
Turn everyday screen demonstrations into structured training content and reusable workplace guides.
Access reusable skills and structured resources that help teams produce consistent content faster.
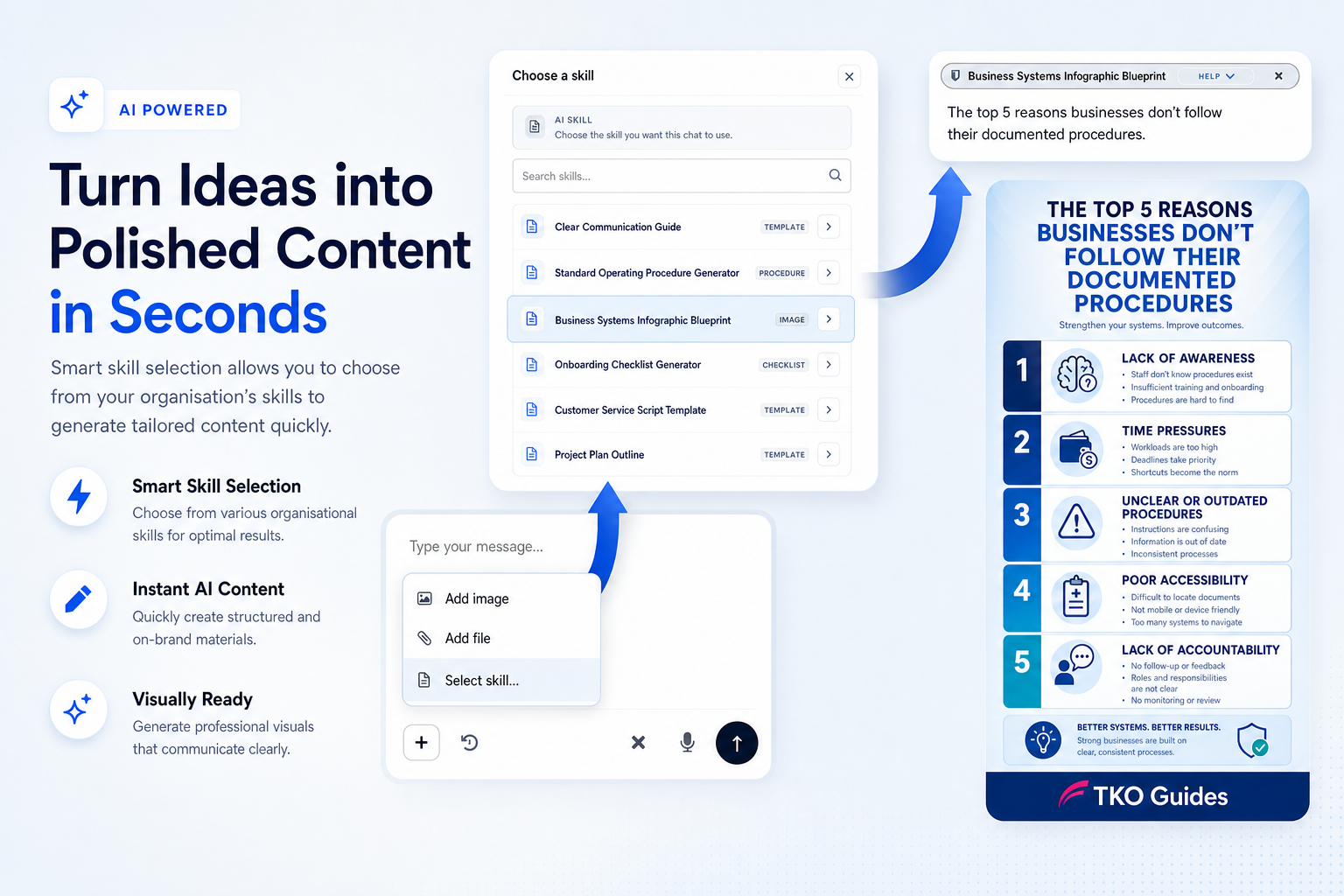
Select the right skill and generate structured, on-brand documents for your organisation.
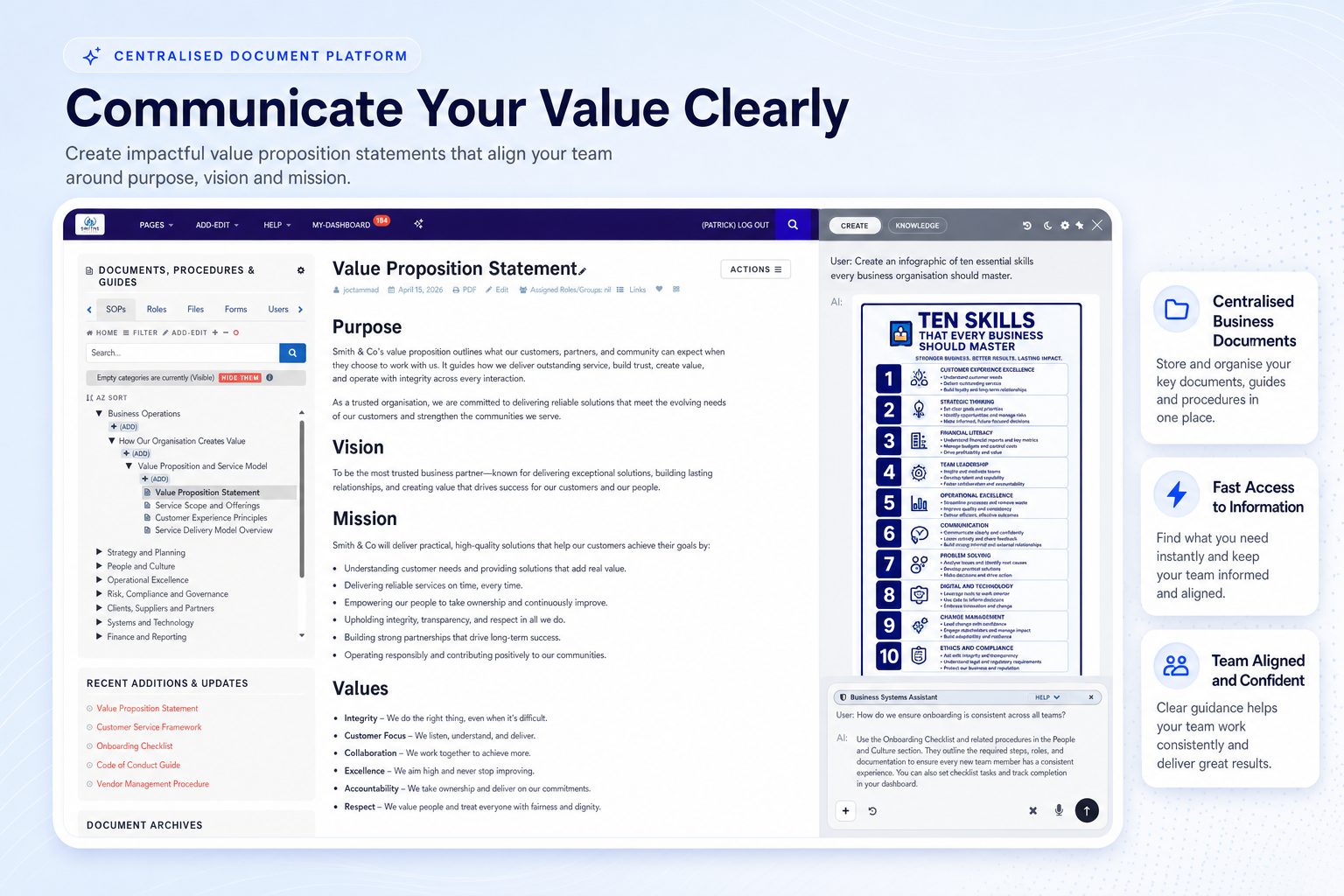
Help teams document service standards, quality practices and everyday operating expectations.
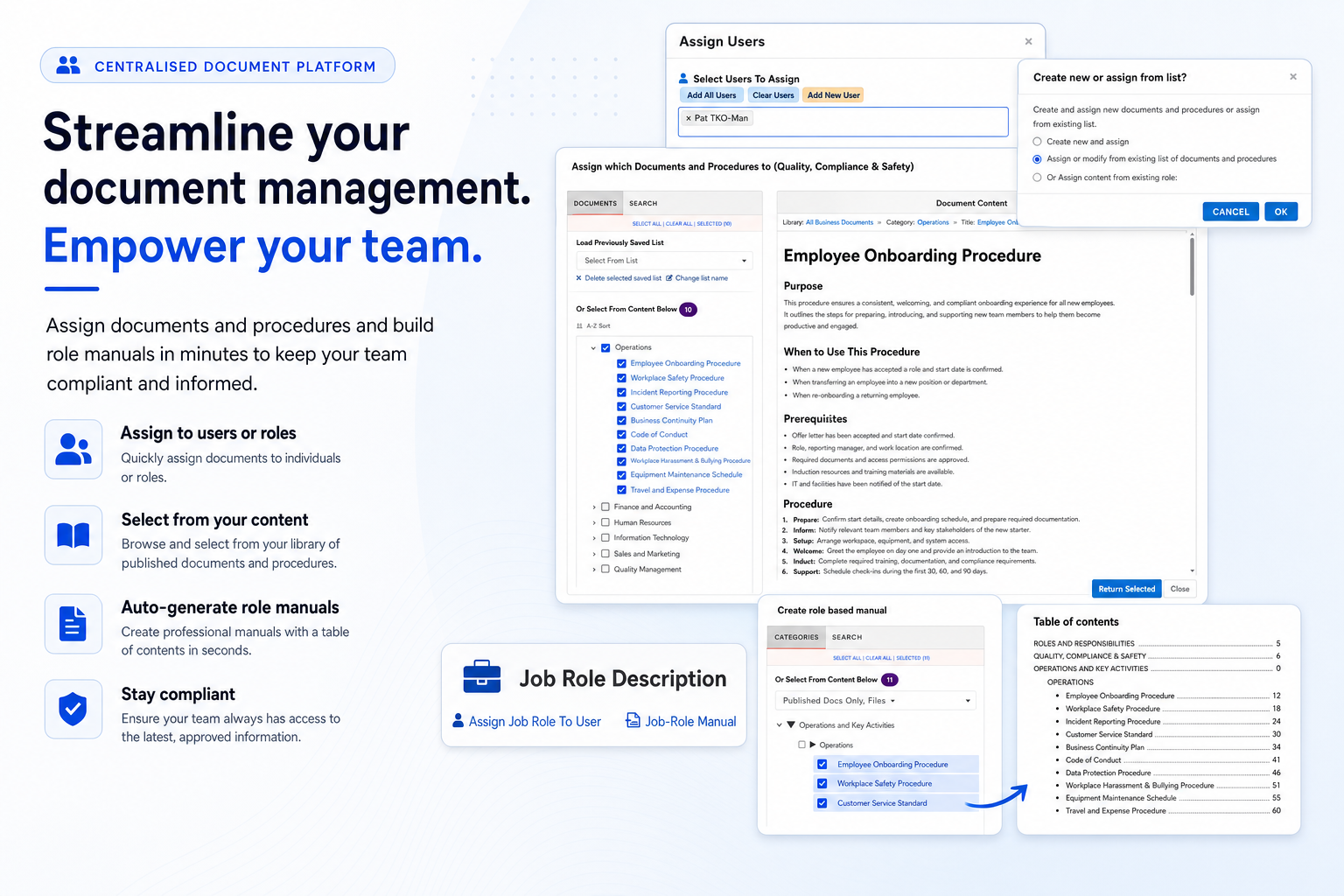
Assign documents by user or role and generate role-specific manuals for faster onboarding.
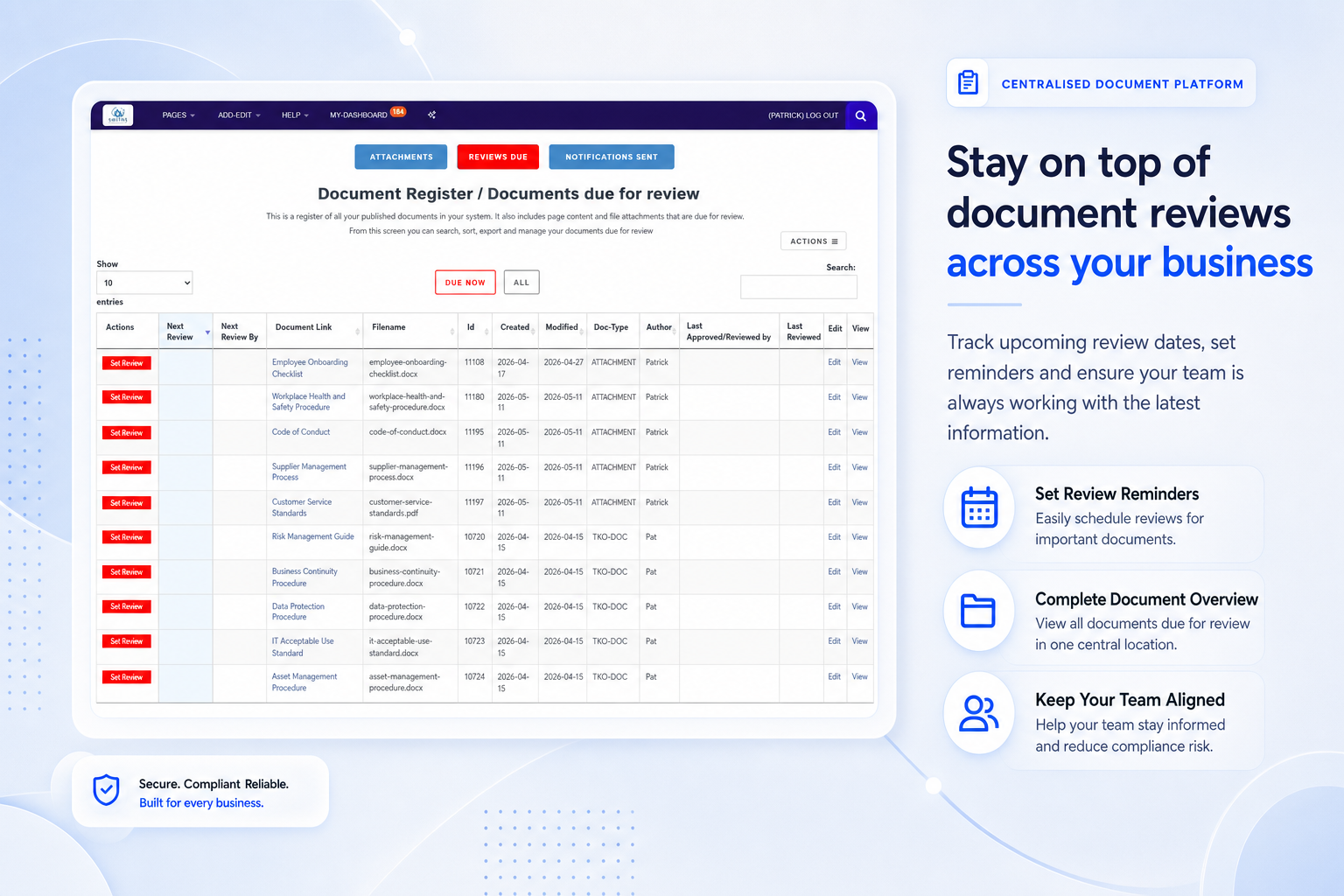
Know what is due, what has changed and where attention is needed before content goes stale.
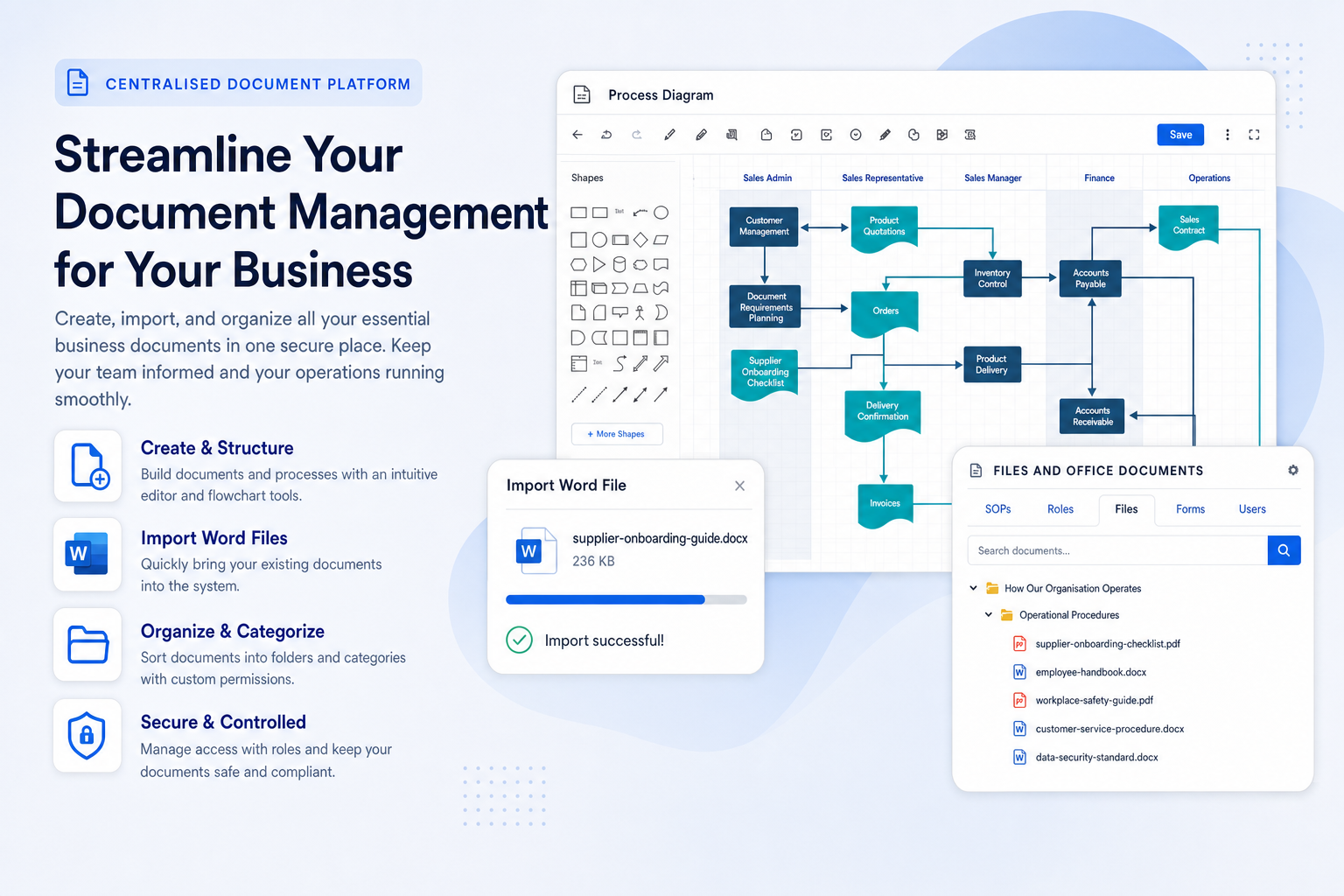
Bring Word files, diagrams, forms and other business documents into one searchable workspace.
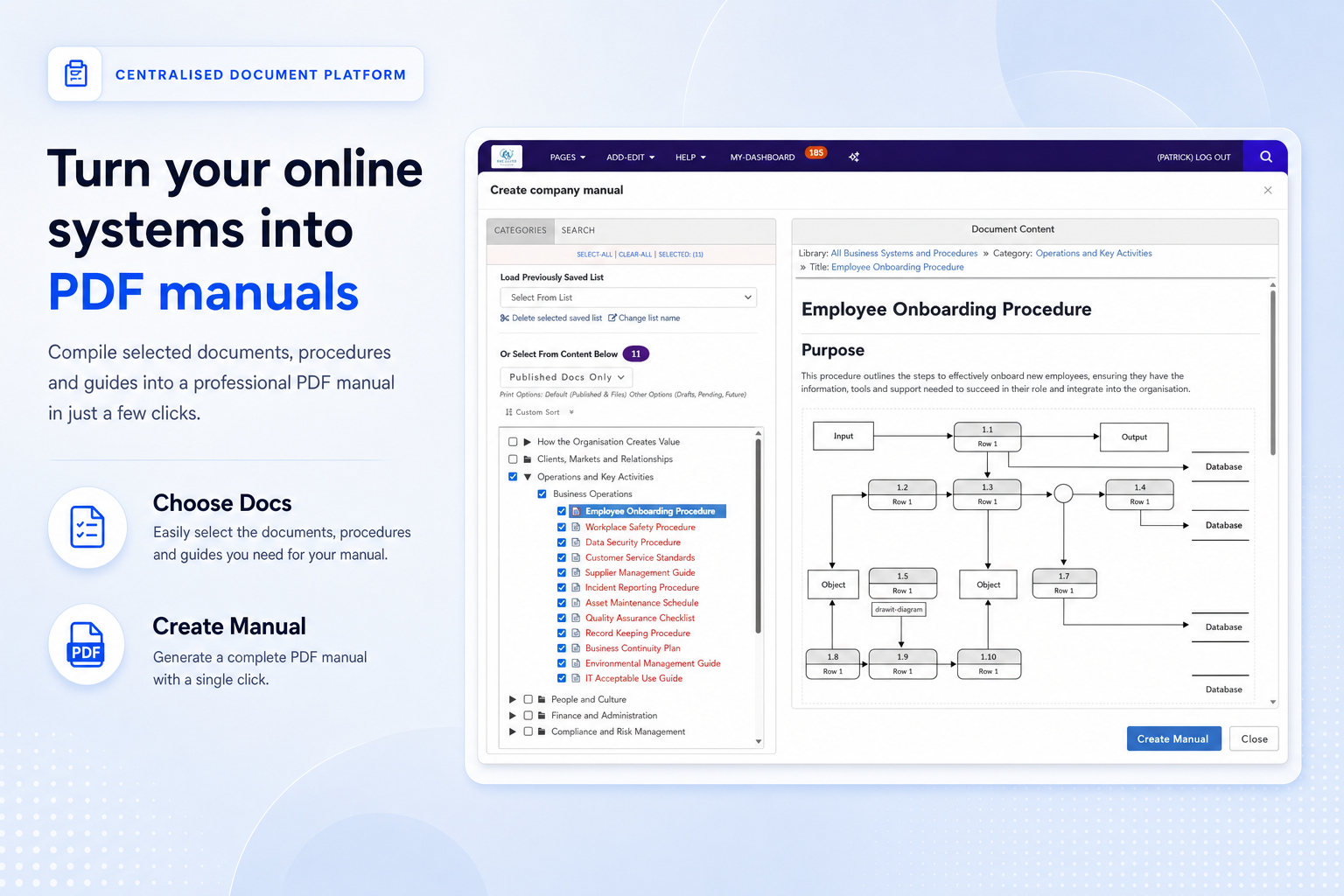
Compile selected documents into professional manuals for staff, contractors, participants or auditors.
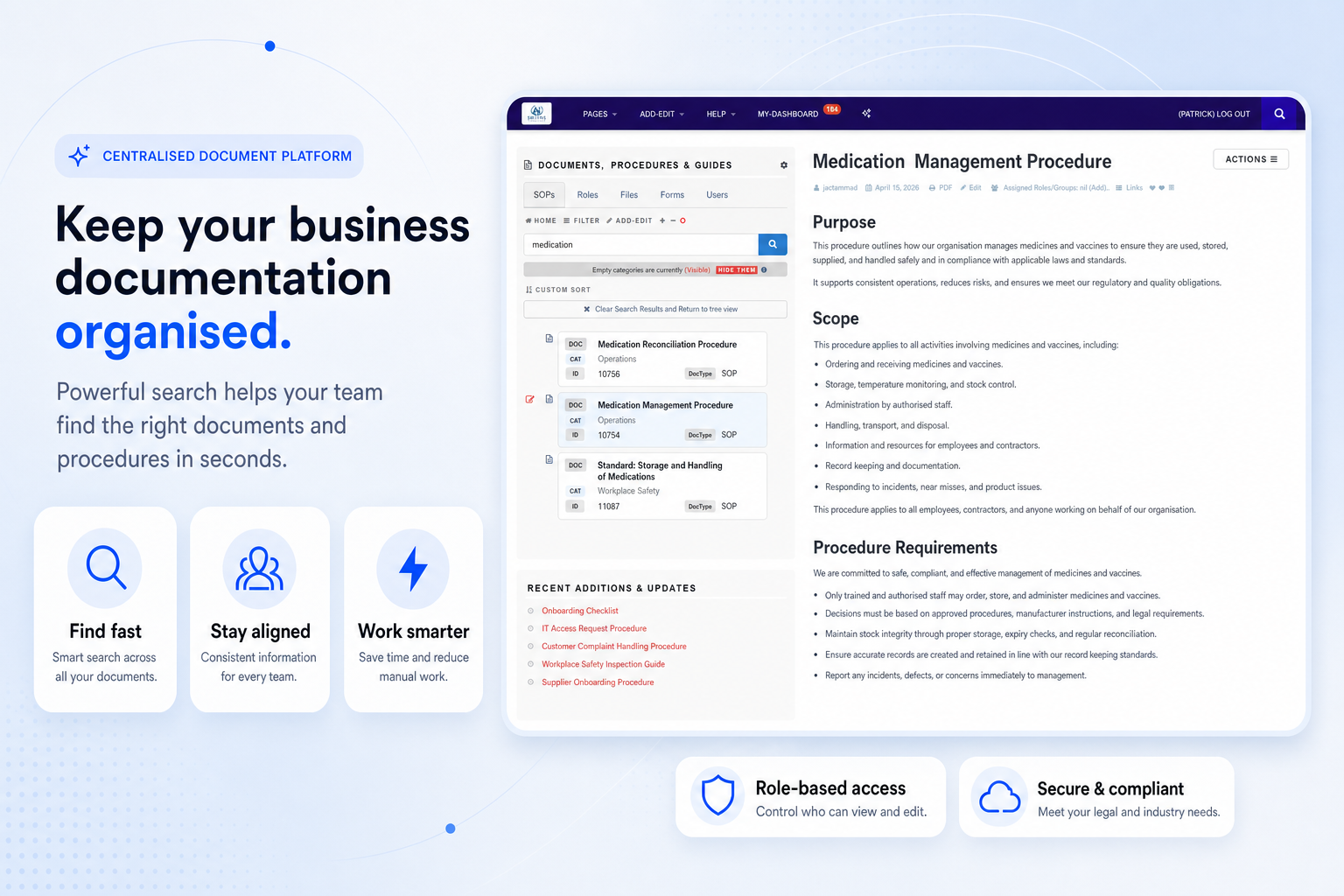
Search across documents and procedures so teams can locate the right guidance in seconds.
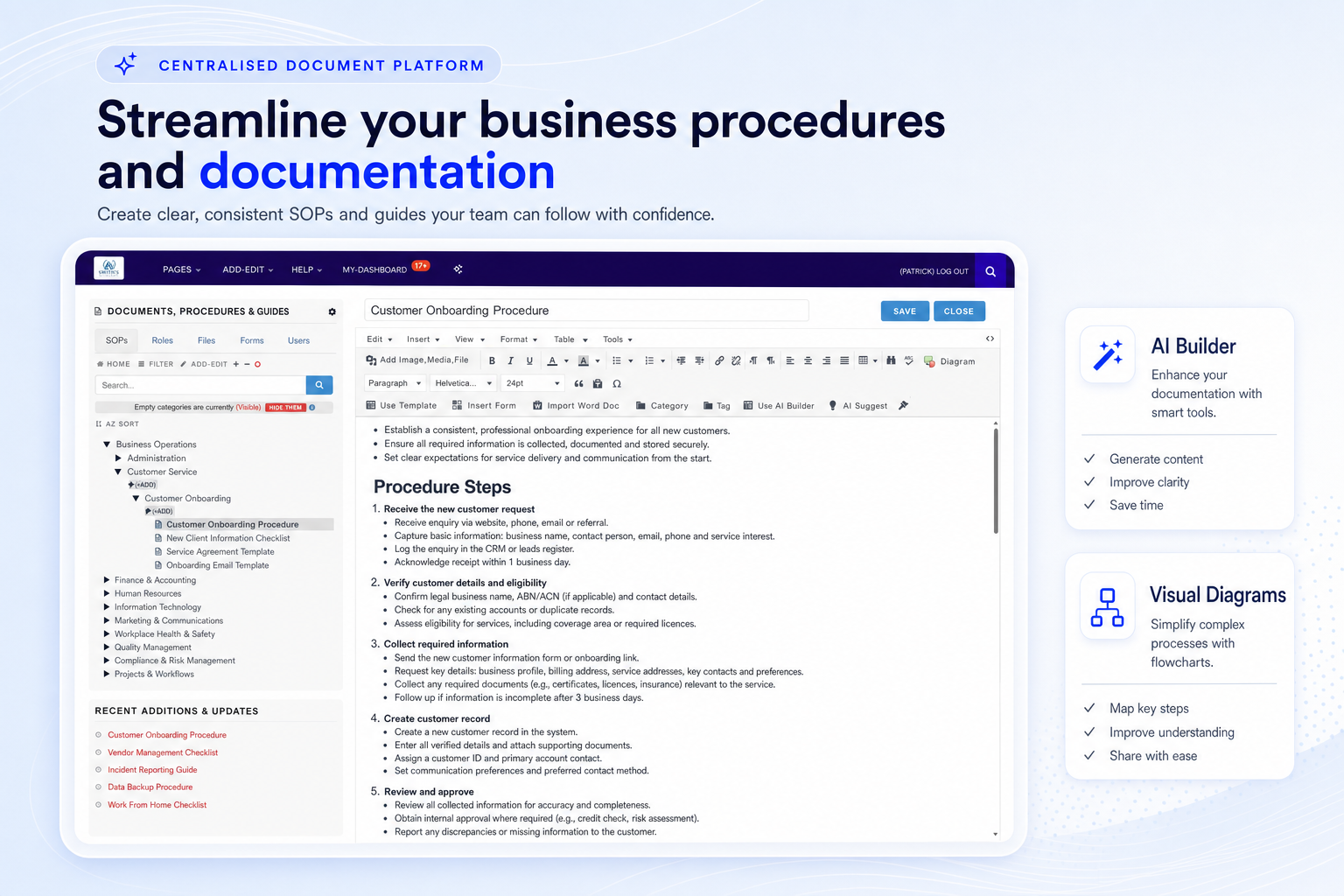
Create and format documents with diagrams, structured content and AI-assisted editing tools.
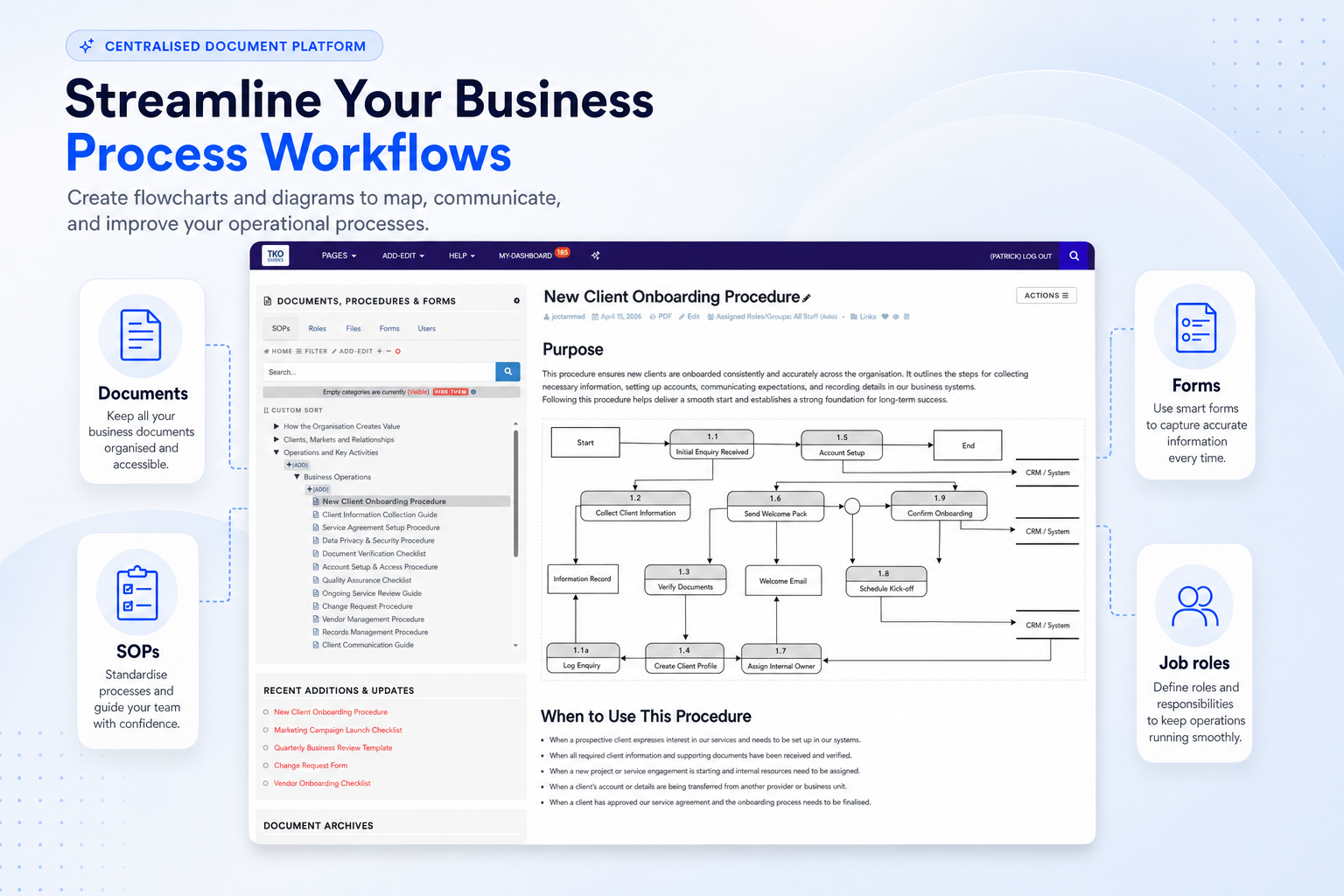
Map registration, onboarding and service delivery steps so everyone understands the process.
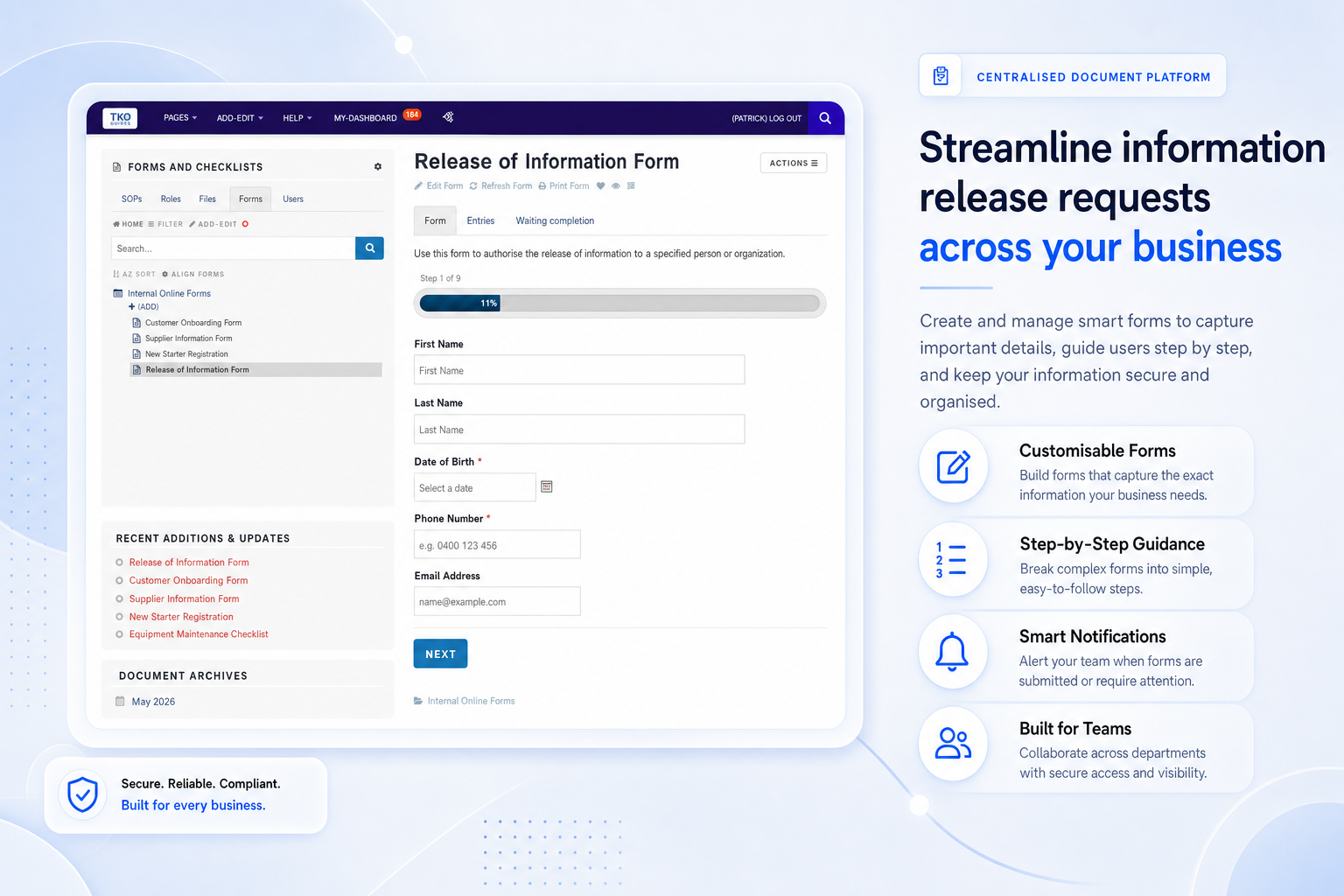
Create secure digital forms that support consistent information capture and document handling.
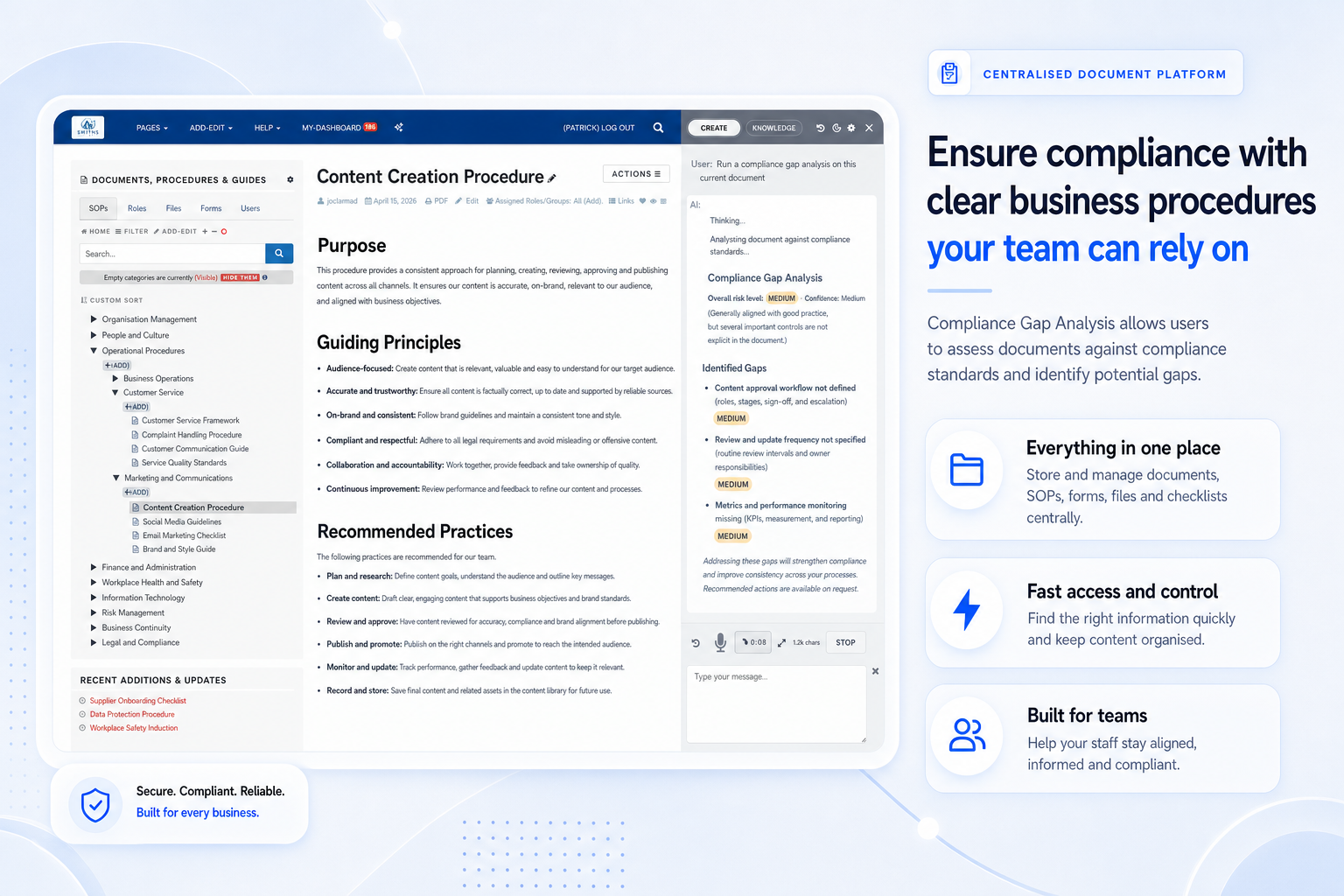
Assess documents against requirements and turn findings into practical improvement actions.
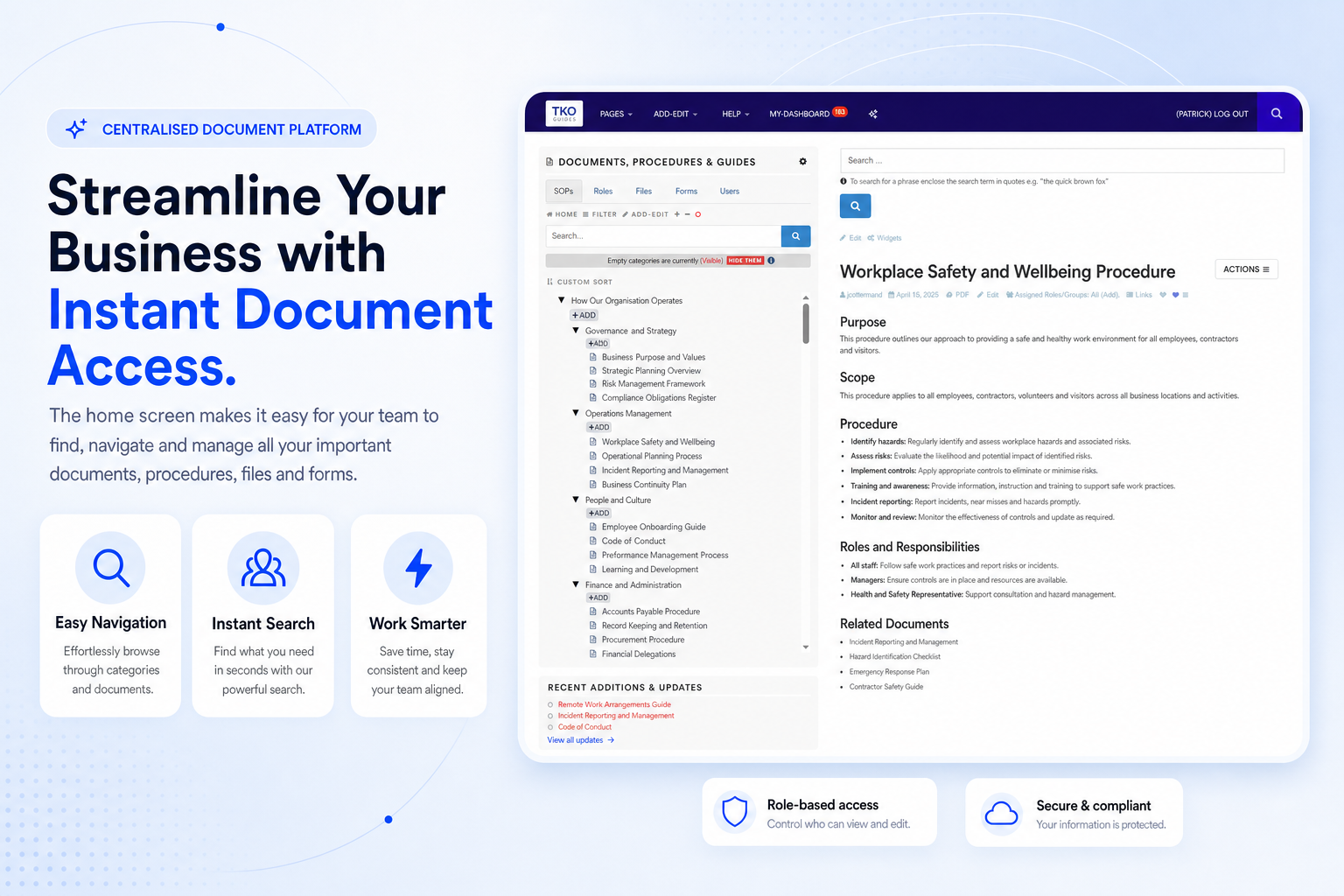
Navigate documents, procedures, forms and files from a clear home screen built for daily use.
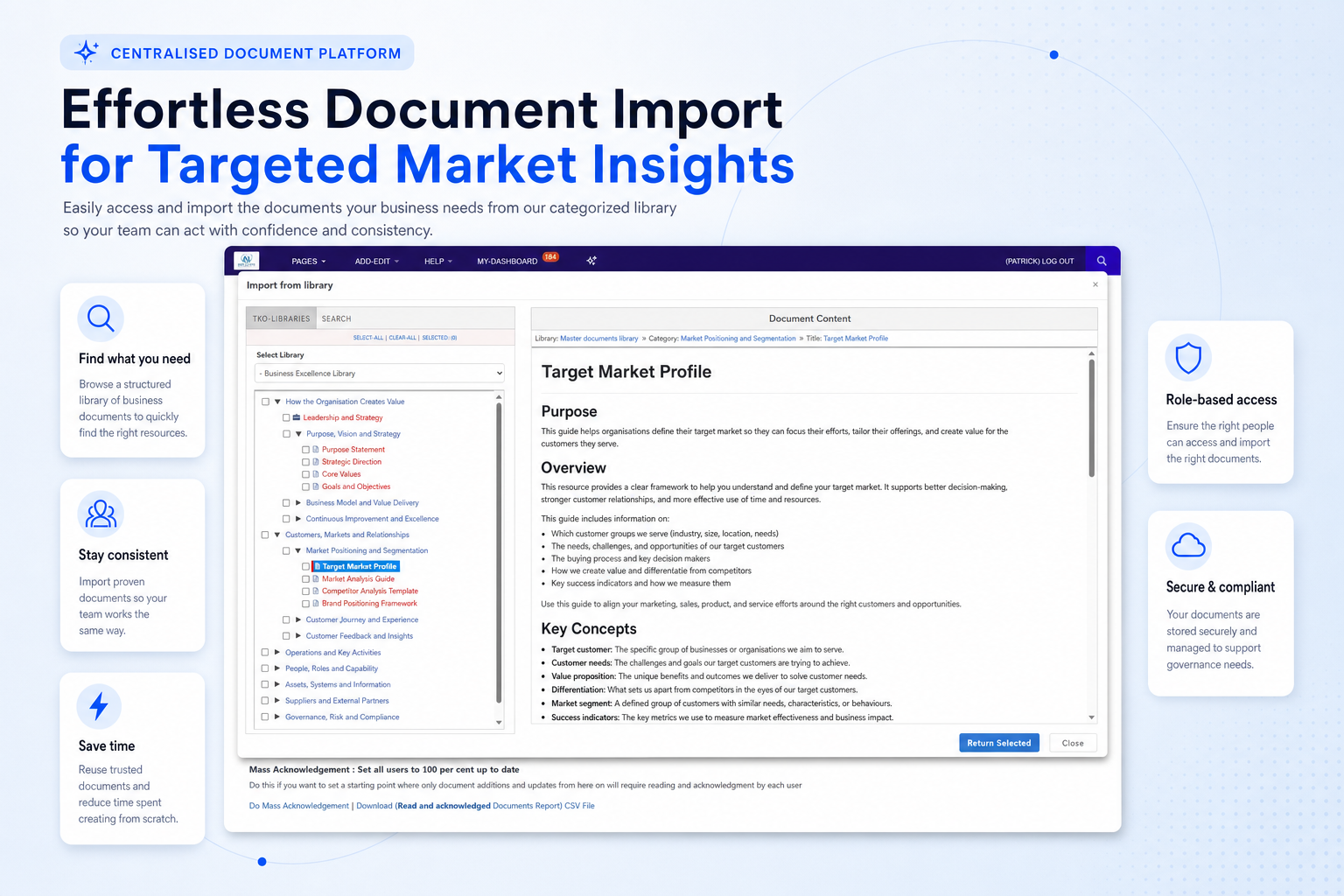
Import selected resources from a categorised library and adapt them to your organisation.
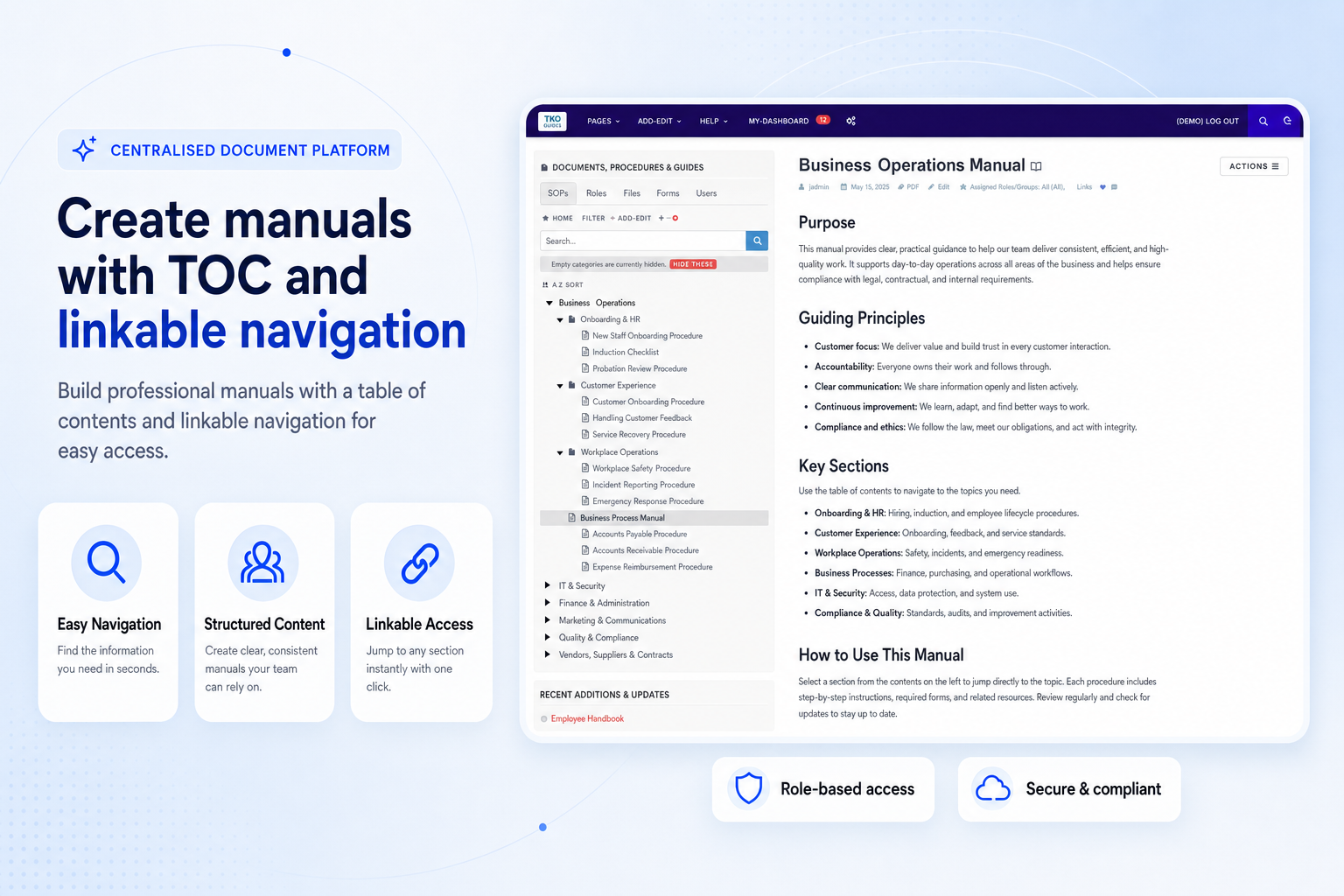
Generate manuals with table of contents and linkable navigation for easy reading.
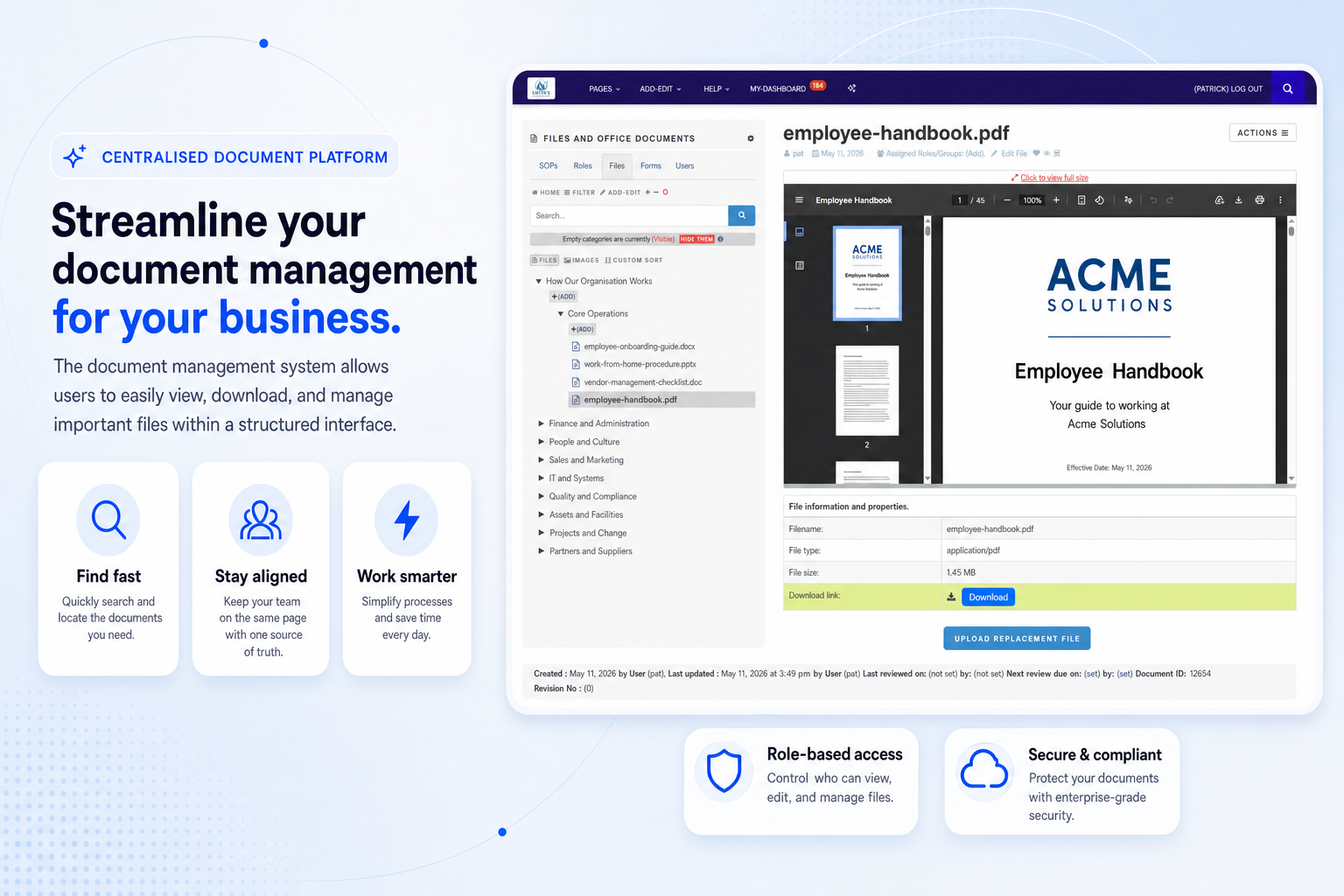
Store, view and download files within a structured interface connected to your document system.
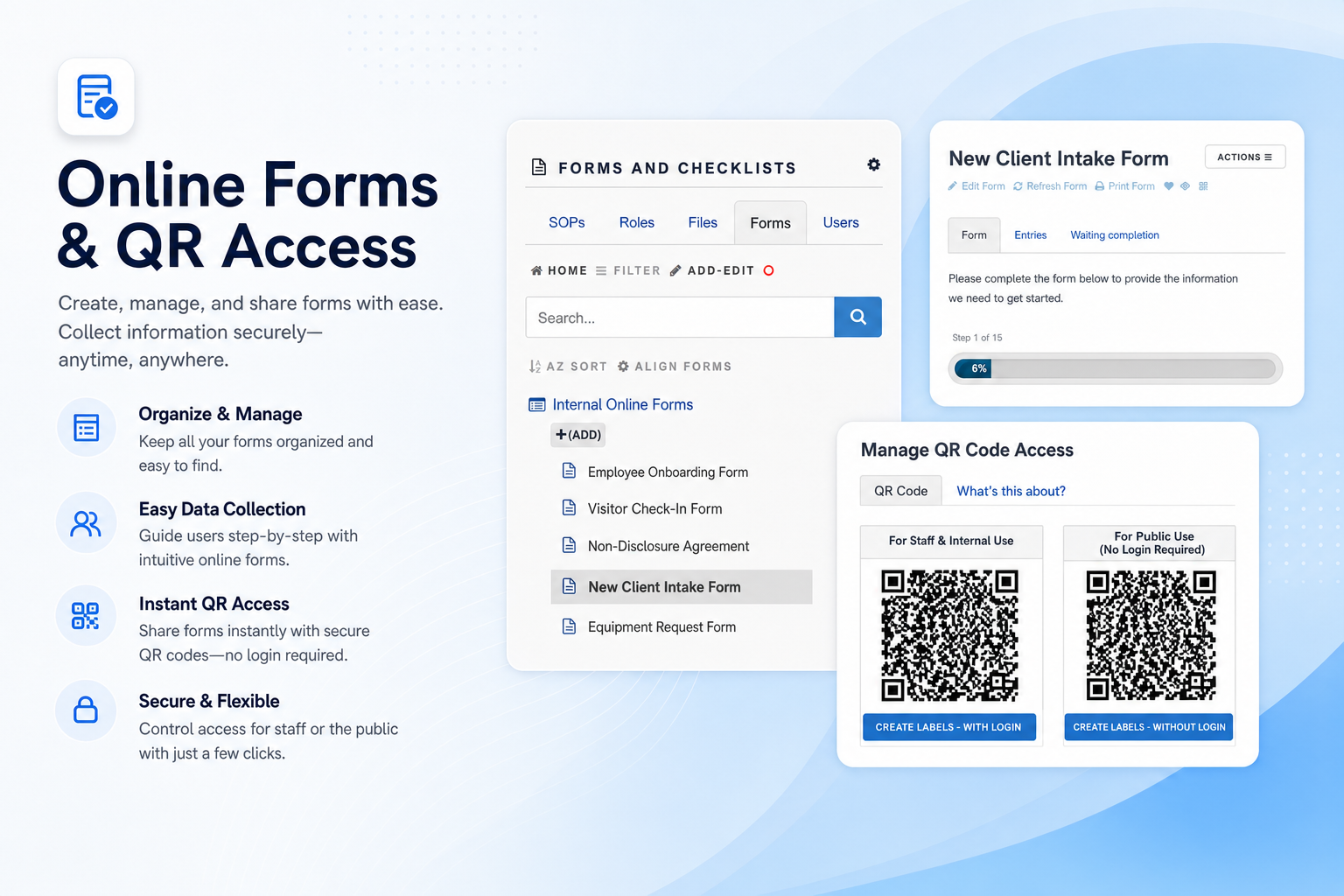
Make secure forms easy to access for staff, clients and participants across devices.
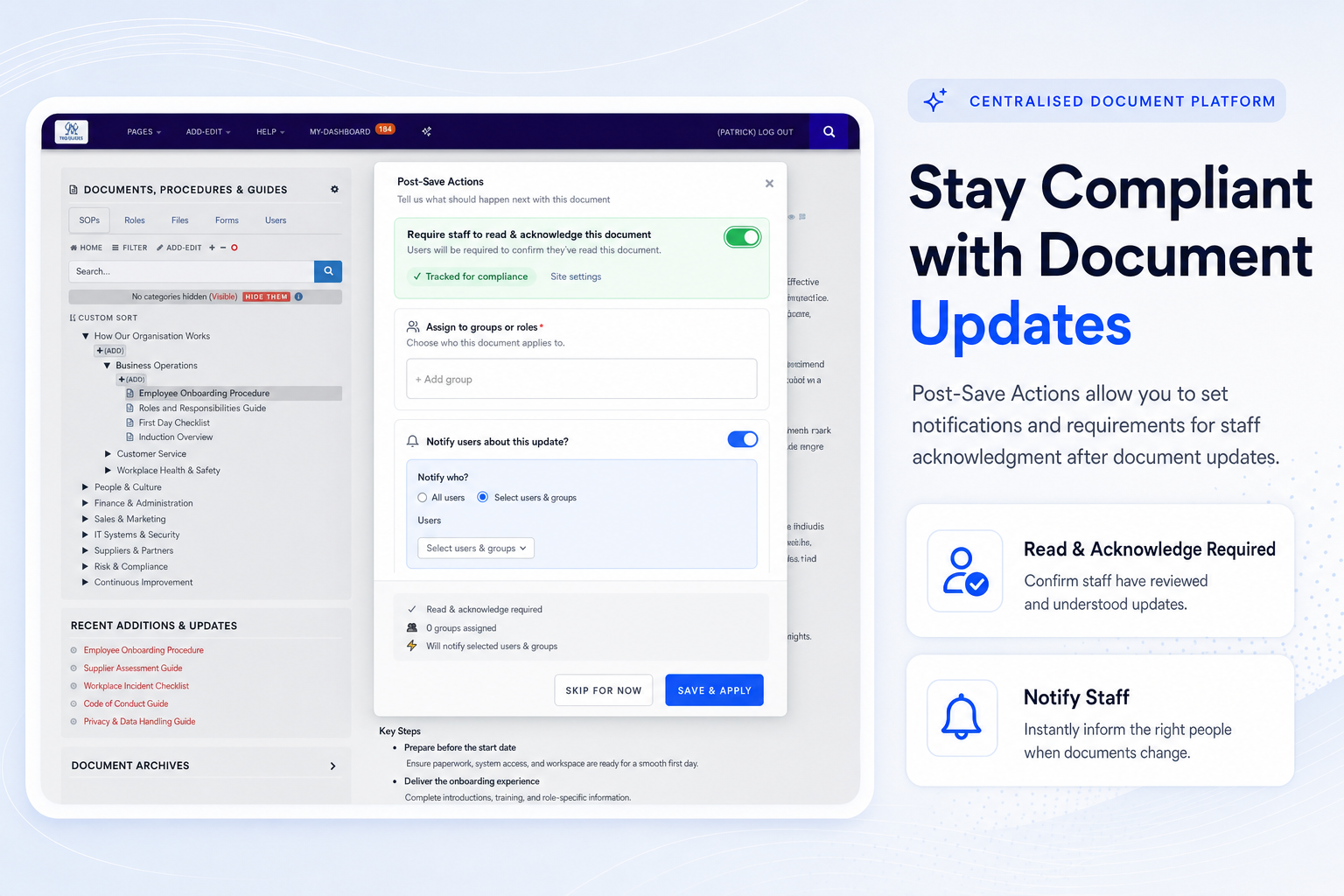
Notify staff, request acknowledgement and reduce confusion when important documents change.
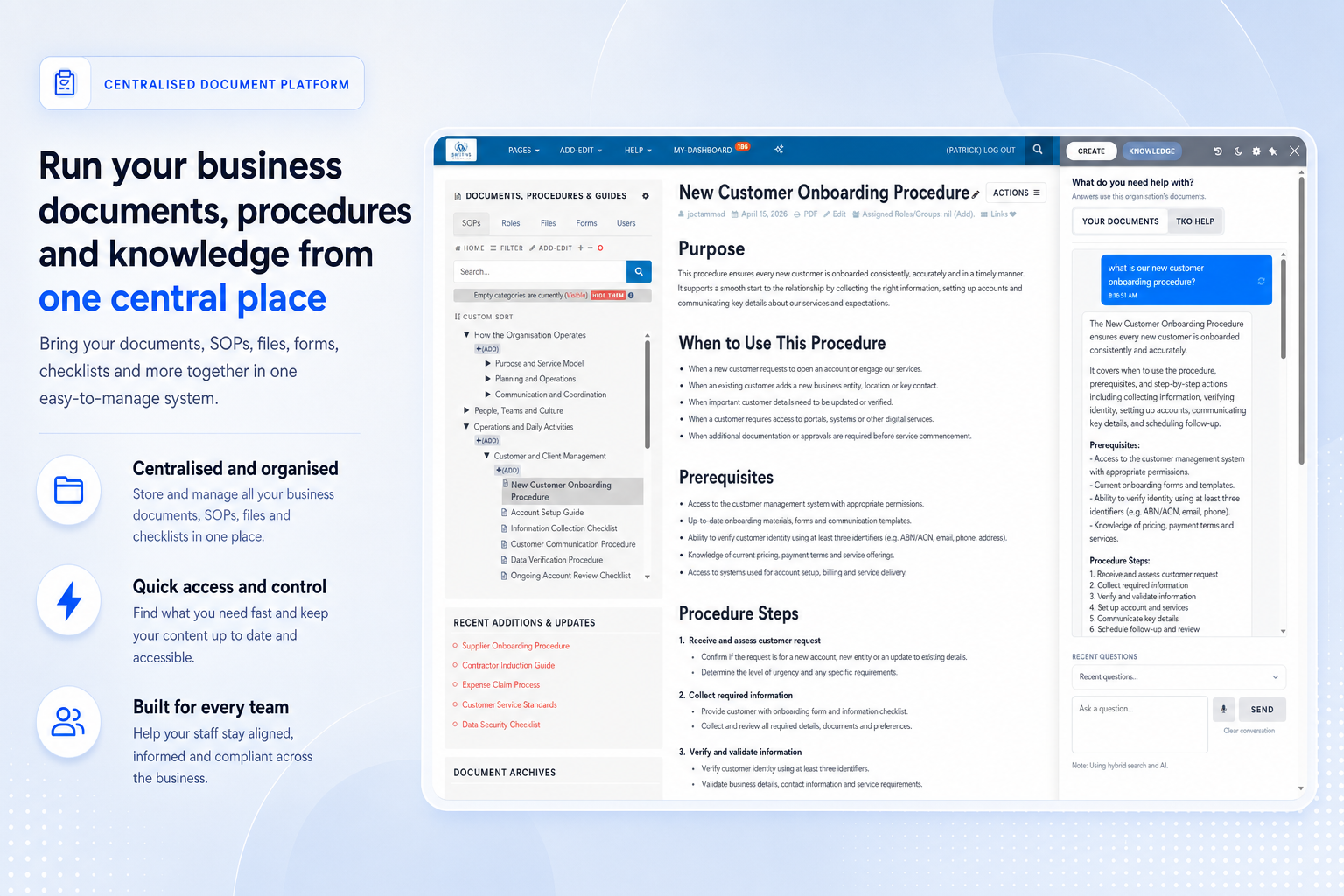
Ask questions against your organisation’s content and help staff find the right procedure quickly.
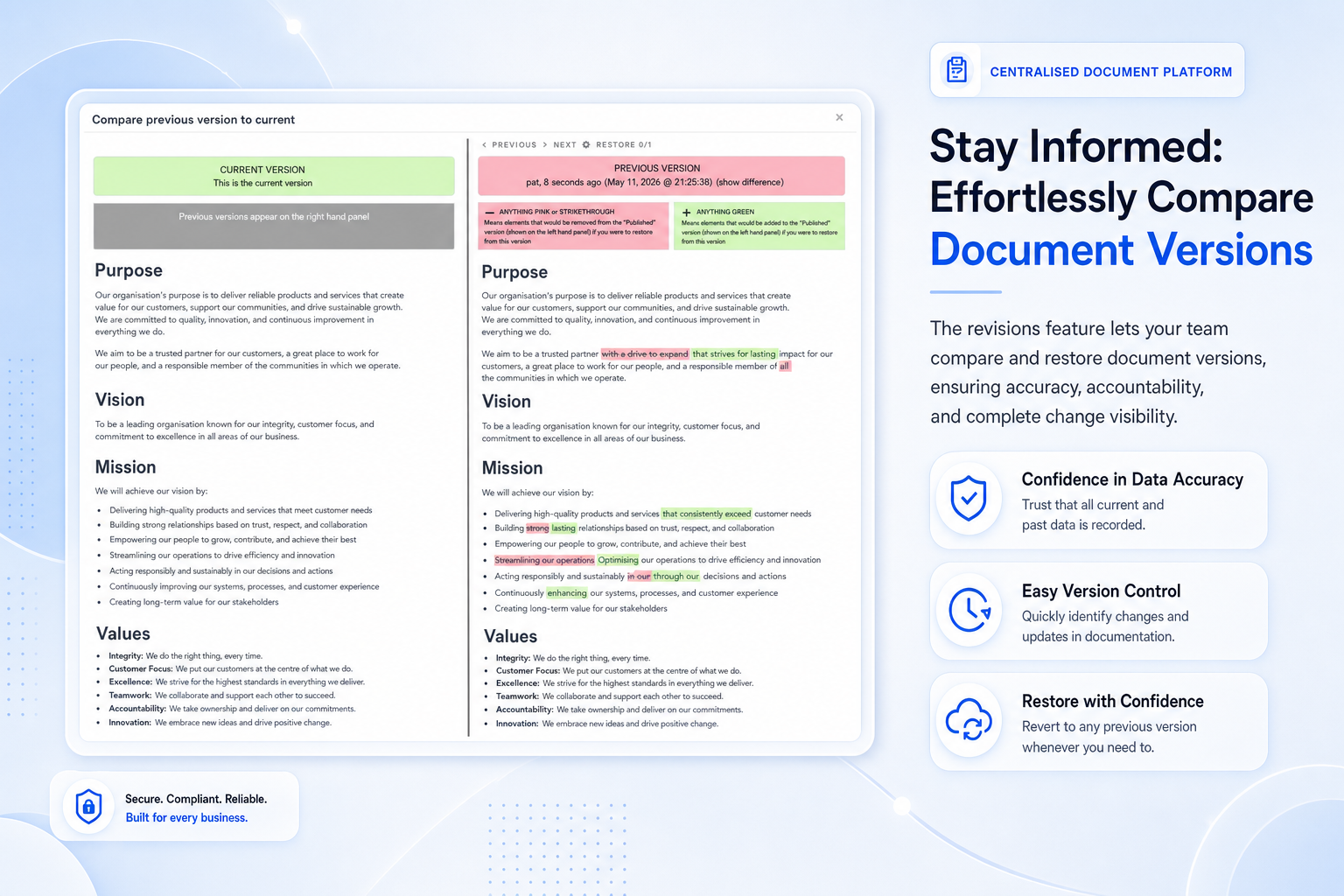
Track changes, restore prior versions and maintain confidence in document accuracy over time.
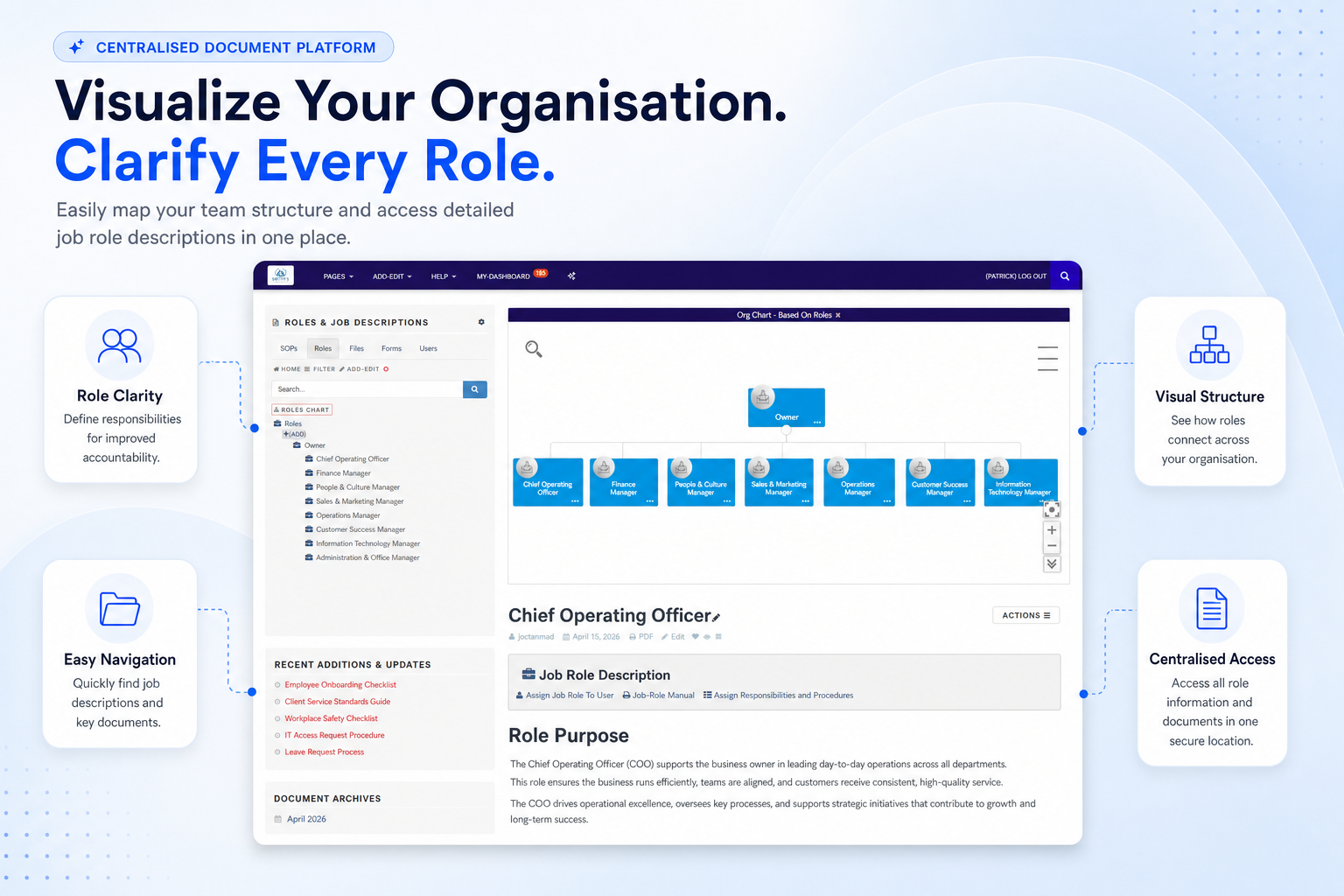
Connect roles, responsibilities and related documents so accountability is easy to understand.
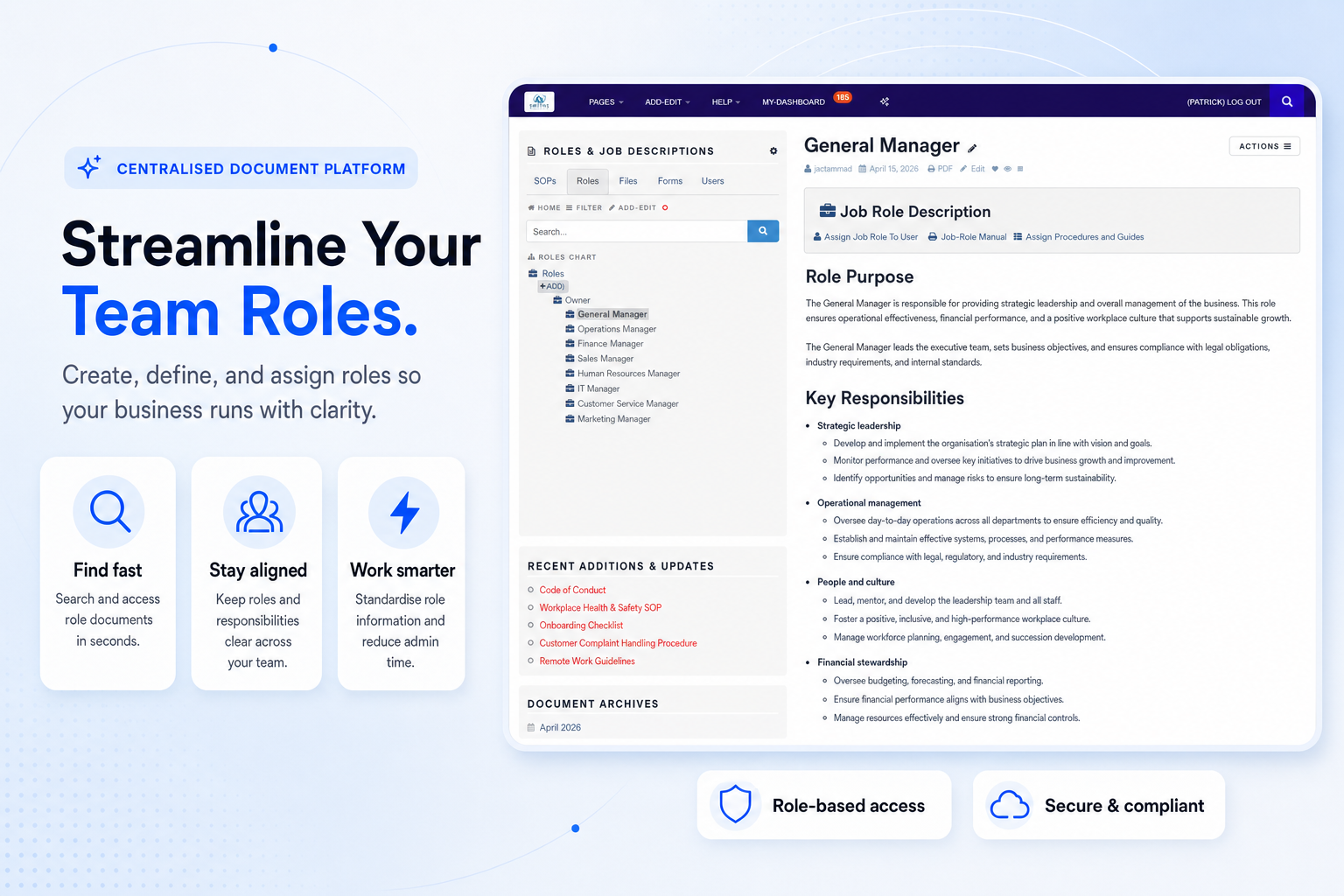
Create roles, assign responsibilities and help staff understand the documents relevant to their work.
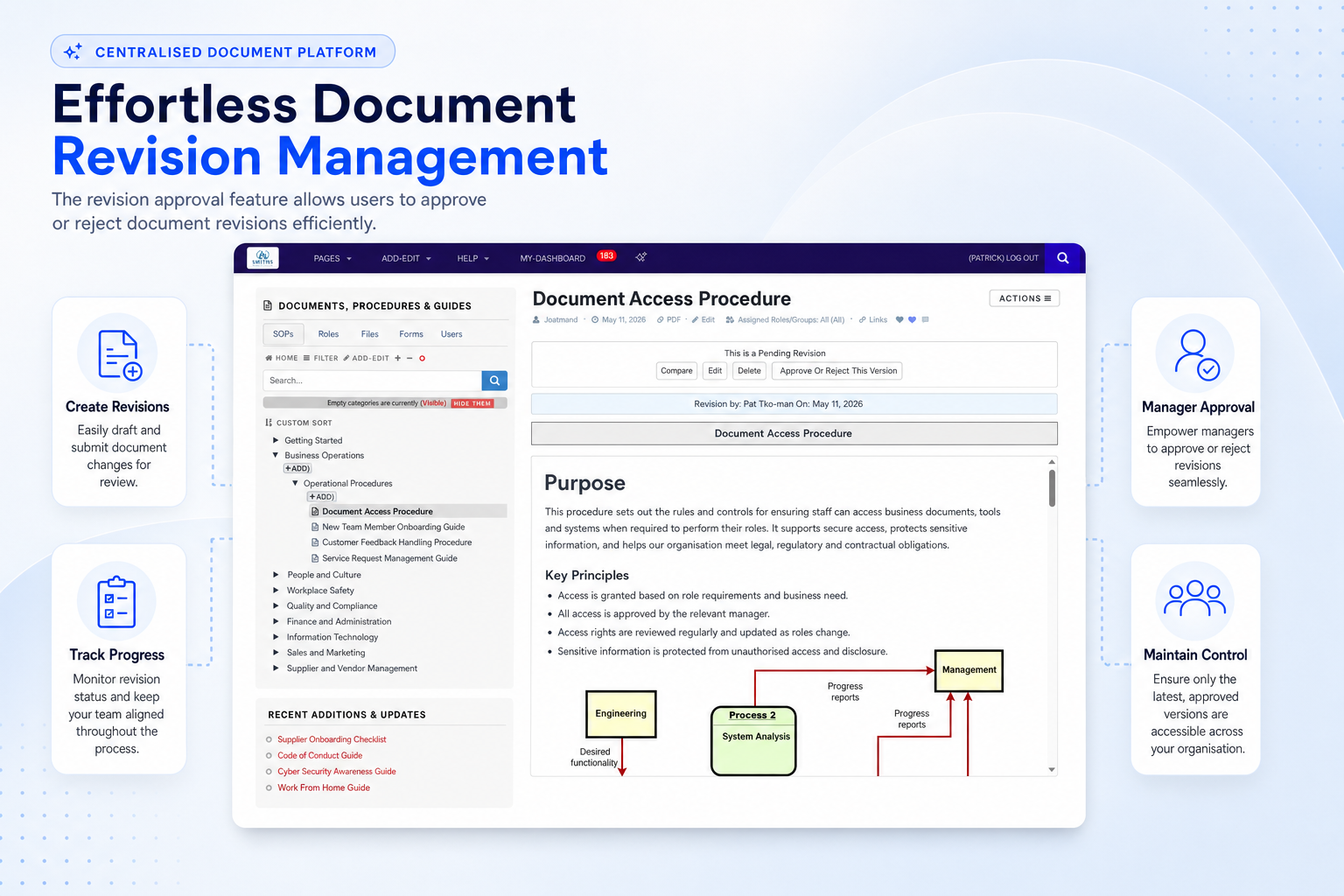
Submit changes for review, approve or reject revisions and keep document governance clear.
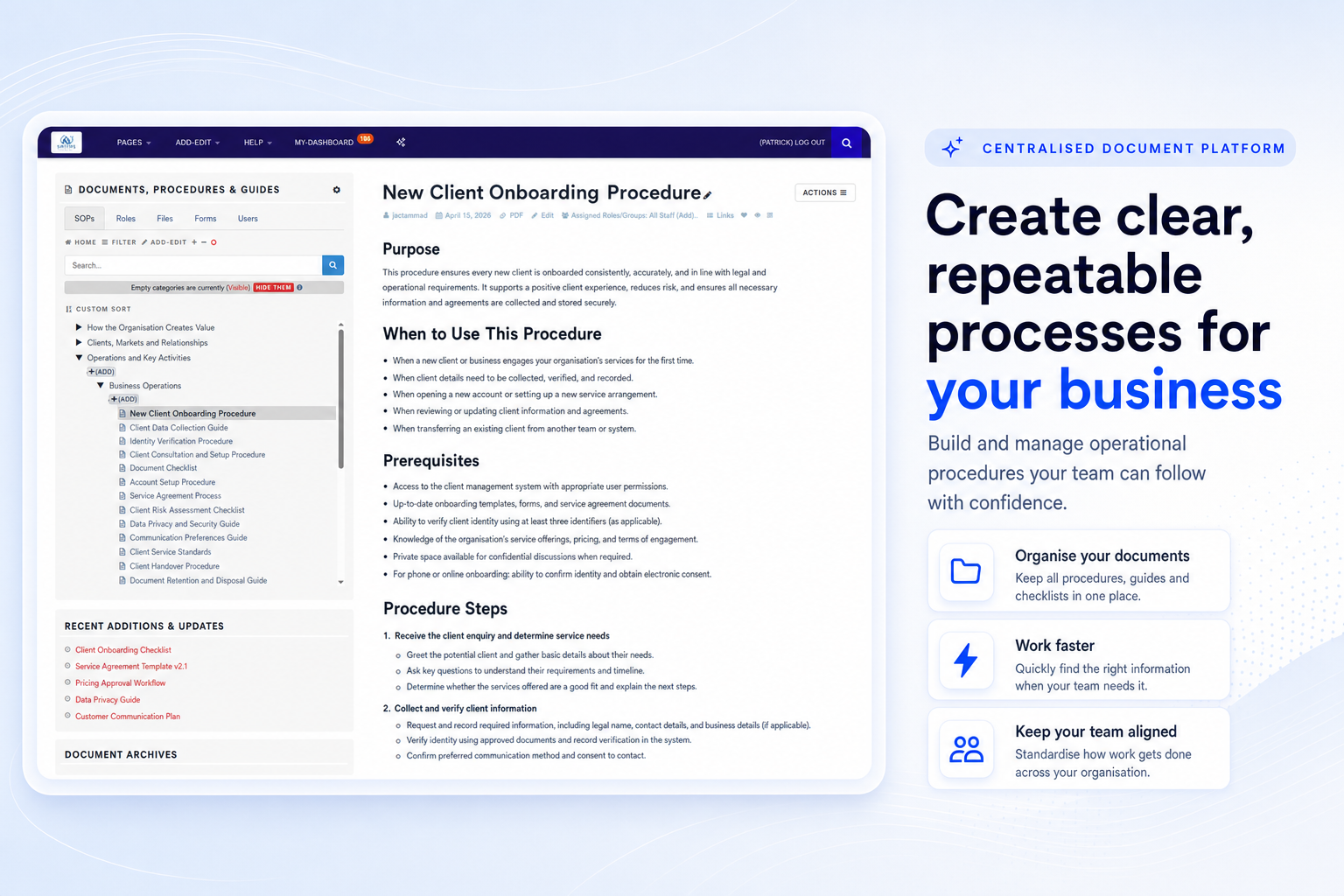
Standardise processes with clear operating documents that support safe, consistent work.
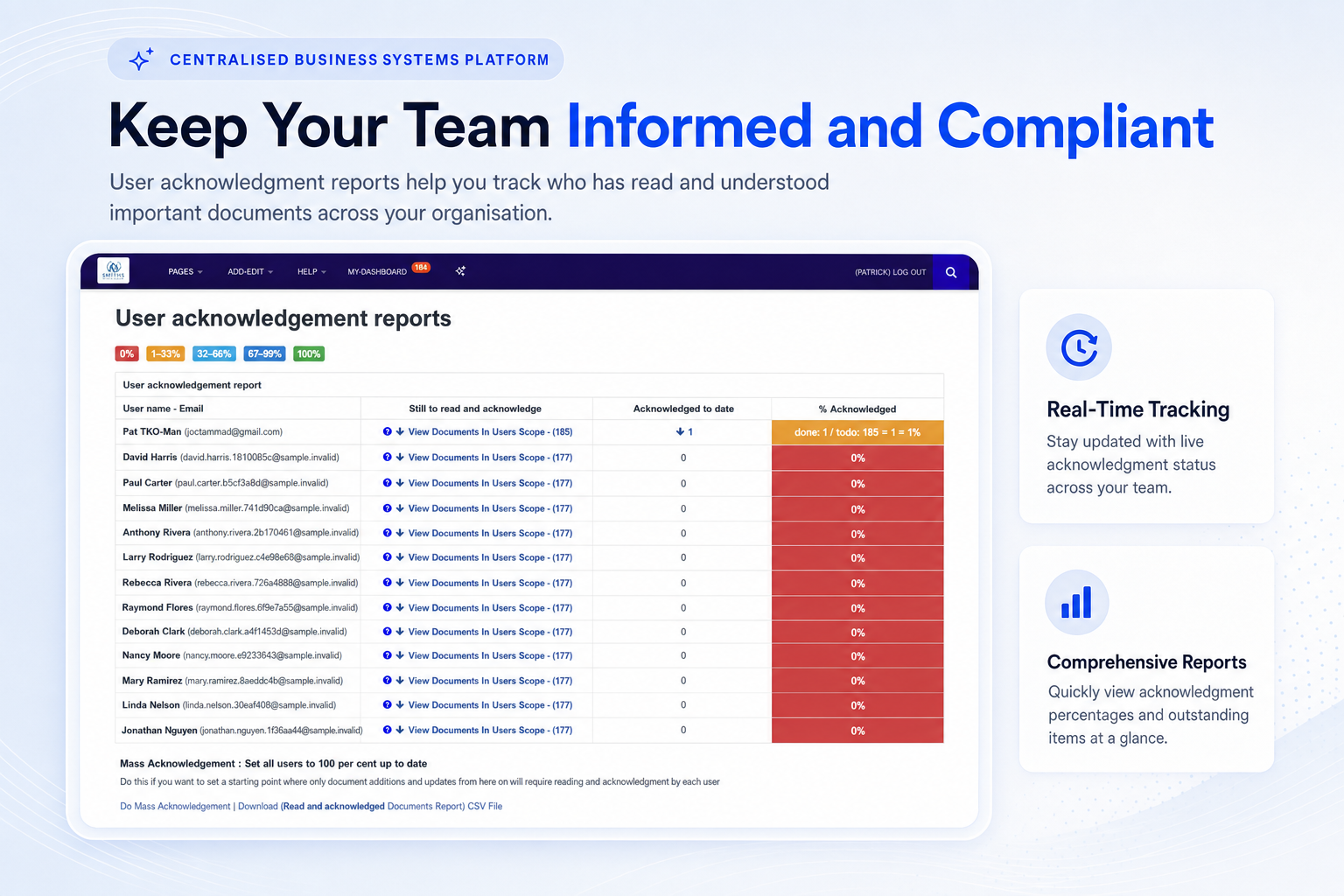
Monitor acknowledgement status and provide evidence that staff have reviewed critical documents.
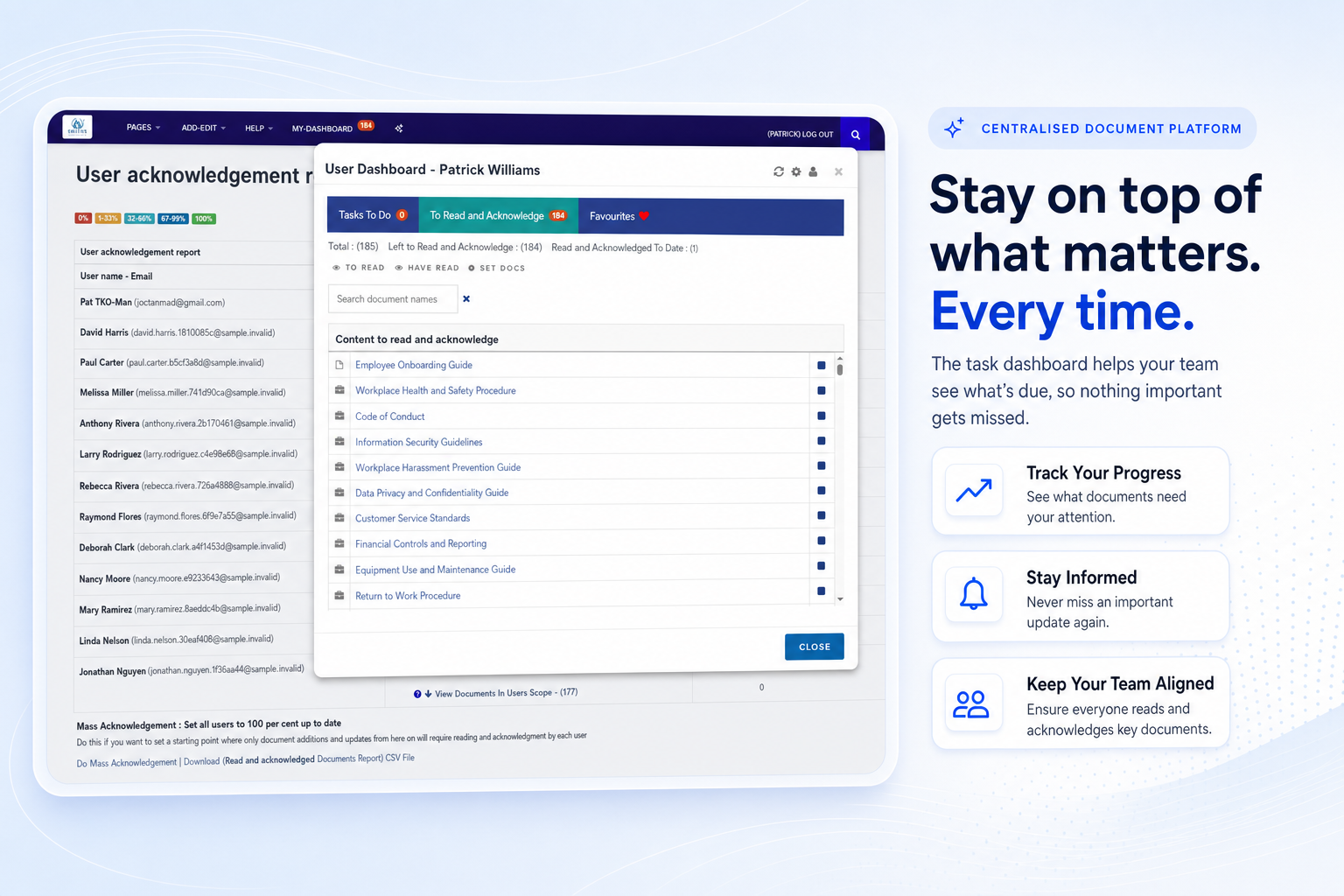
Give users a simple dashboard for pending reading, acknowledgements and review tasks.
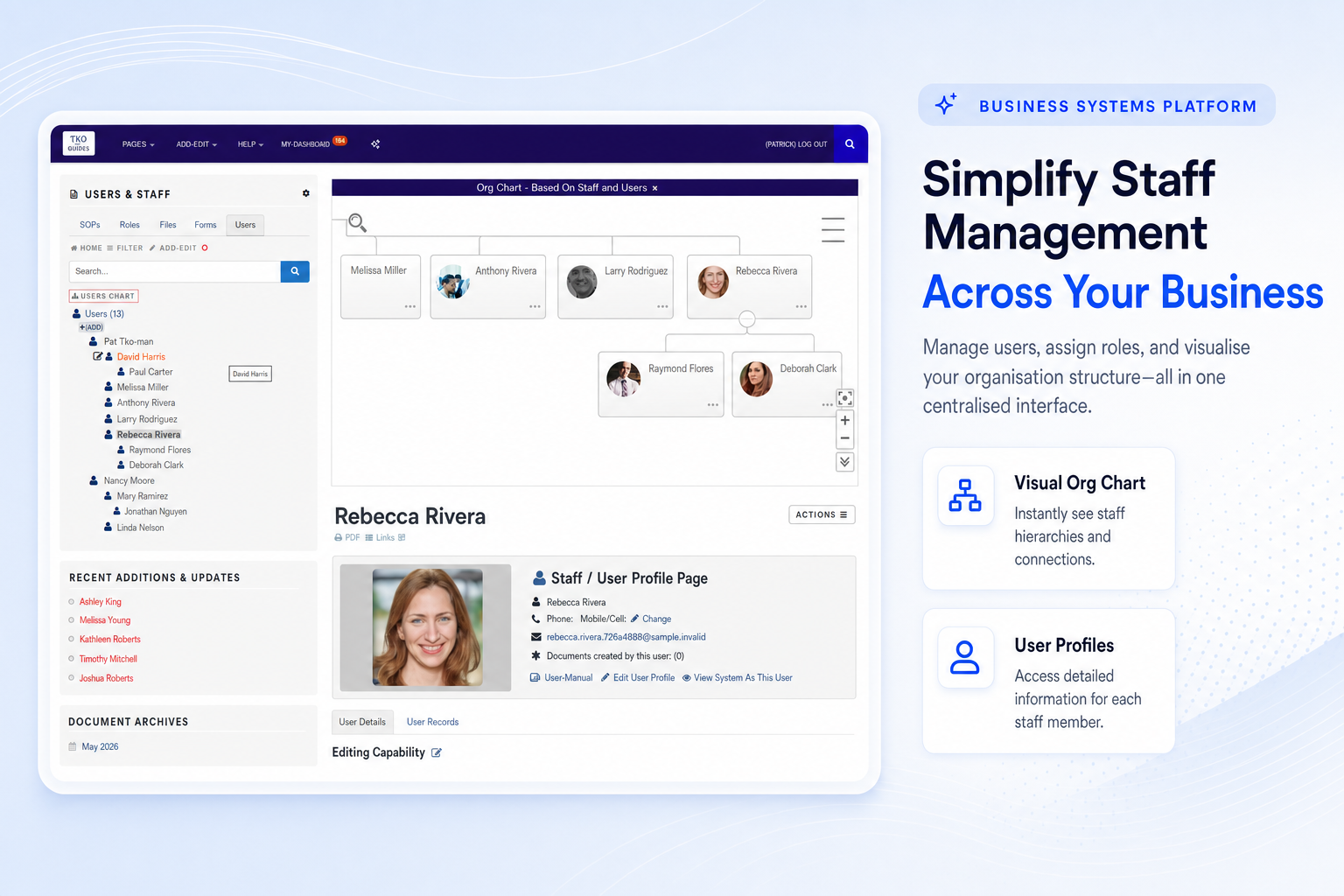
Manage users, roles and structure so the right people can access the right documents.
Designed for organisations that need reliable documentation without adding unnecessary administrative weight.
Keep procedures, forms, guides and audit records connected to the way your teams actually work.
Replace fragmented folders and old attachments with a clear source of current information.
Give new starters role-based manuals, assigned reading and practical guidance from day one.
Use review histories, revisions and acknowledgements to retrieve evidence with less stress.
Operational leaders use TKO Guides to bring clarity, consistency and control to business-critical documents.
“Having documents, review dates and evidence in one system makes quality management far easier to maintain. It gives our team a practical way to stay aligned.”
“The structure helps remove guesswork. Our procedures are easier to find, easier to update and much easier to explain during internal reviews.”
“For operations teams under compliance pressure, a controlled document system is invaluable. It helps keep standards visible and responsibilities clear.”
Here are the practical questions organisations often ask when moving from scattered documents to one managed system.
Yes. TKO Guides is well suited to NDIS providers that need to organise procedures, forms, service documents, staff guides and evidence for internal reviews or audits.
Yes. You can bring existing files into the platform, organise them into a structured library and improve them over time using review tools and AI-assisted workflows.
Role-based manuals, assigned documents and acknowledgement tracking help new team members understand expectations faster and reduce reliance on one person’s memory.
TKO Guides is designed for secure access across modern devices, helping distributed teams find current guidance without digging through disconnected folders.
You can update documents, track revisions, notify staff and retain evidence of acknowledgements so changes are communicated clearly.
Book a demo to explore how TKO Guides can centralise documents, reduce manual follow-up and help your organisation stay audit-ready.
Book a DemoReach out to TKO Guides or book a demo at a time that suits you.
See how the platform can support your document library, reviews, assignments and audit evidence.
Phone: 1300 498 180 or (int) +61 419337287
Email: pat@tkodocs.com